Leeham News and Analysis
There's more to real news than a news release.
 Leeham News and Analysis
Leeham News and Analysis
- Bjorn’s Corner: New engine development. Part 4. Propulsive efficiency April 19, 2024
- Boeing unlikely to meet FAA’s 90-day deadline for new safety program April 18, 2024
- Focus on quality not slowing innovation, says GKN April 18, 2024
- Boeing defends 787, 777 against whistleblower charges April 17, 2024
- Dissecting Boeing CEO’s statement next new airplane will cost $50bn April 15, 2024
Bjorn’s Corner: Can I get COVID-19 in airline cabins? Part 1.
May 8, 2020, ©. Leeham News: In our Corner series, we now dig into this important subject: Is my probability of getting infected with the COVID-19 virus higher in an airliner cabin than in other places?
We look at simulations of how the virus travels when we breathe/cough and how the virus load propagates in an airliner cabin. Then we talk about infection probabilities compared with other environments.
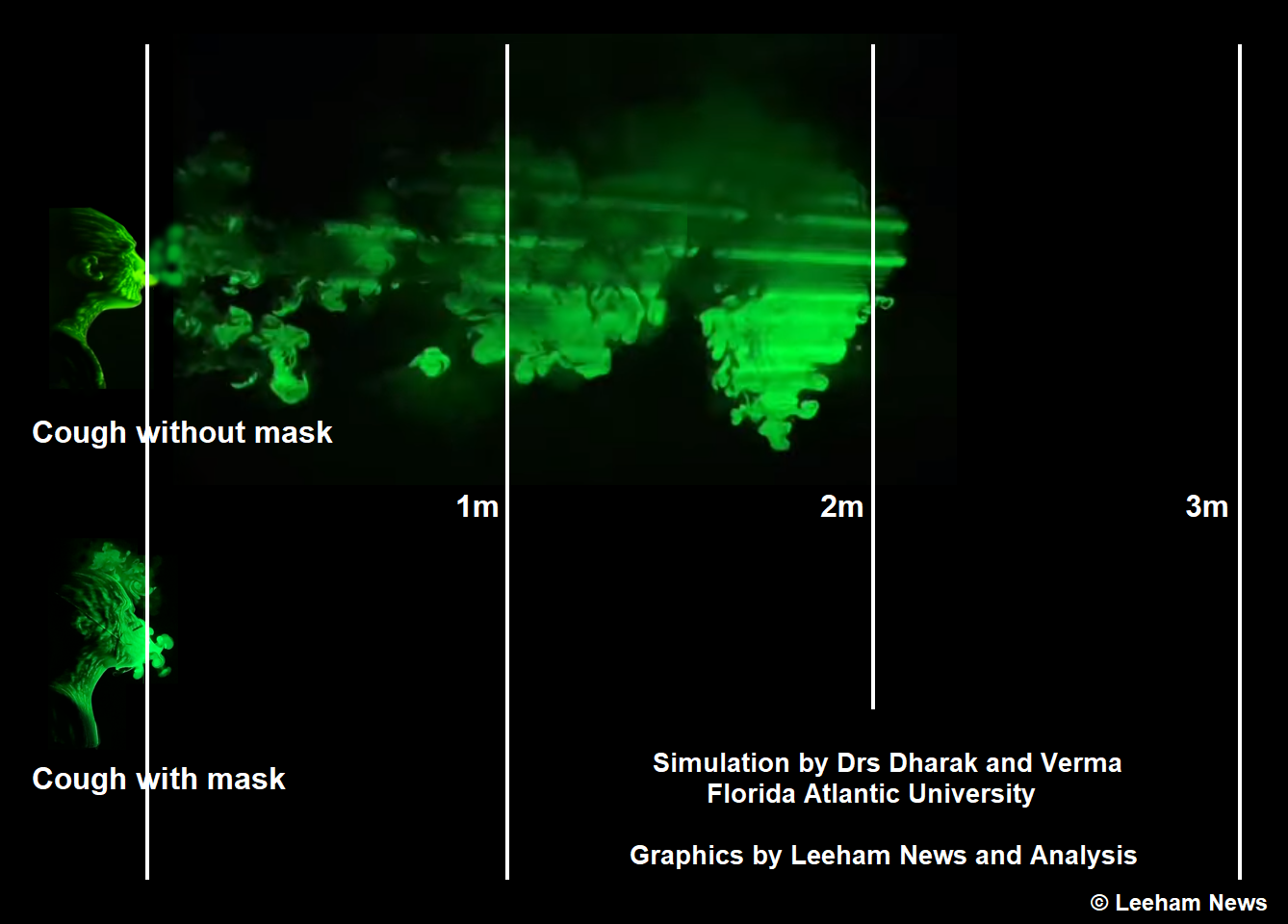
Figure 1.
What are the spreading mechanisms of COVID-19?
The scientists are sure the main infection path is when inhaling droplets coming from exhaled breathing air from an infected person.
Recent simulations by Florida Atlantic University using a simulated aerosol with the smaller and more dangerous droplets (10 to 20 microns in size) show the finer droplets travel up to 3m (10 feet) after a cough, and these can hover in the air for a minute after the cough. Figure 1’s upper part shows the beginning of this process (the stripes in the cloud are from laser lighting effects).
The Florida Atlantic University video with different cough simulations is here.
We got the right to show the simulations and asked Professor Dharak to make a simulation with a face mask. The difference is dramatic, Figure 1 lower part.
The virus can also survive a day or more on a non-porous surface (to not dry out so fast) like a metal handle or our mobile phones. To be infected, the virus must then be brought to our nose, mouth, or eyes by our hands, and there enter our tissues.
This is why regular handwashing is so important and why handwashing or rinsing hands with alcoholic gel after touching public surfaces are recommended.
The probability of getting the virus to the lungs where they can cause a dangerous infection is much higher through the aerosol path than the touch path. There is still no clear evidence of a touch path infected patient, according to the experts.
When flying on an airliner post-COVID, both paths are in focus.
The droplet/aerosol path
The danger of inhaling infectious droplets/aerosol depends on how far it travels from the infected person and how long it stays airborne. In areas without a directional airstream displacing the droplets/aerosol from our breathing level, the risk is higher. Figure 1 is such a case.
Examples thereof are any indoor confinements like shops, stations, trains, buses, work areas, and airport check-in or waiting areas.
Airliner cabins do not count to this category. The Environmental Control System preparing the air we breathe in aircraft builds on a directional airflow from top to bottom. The flow, which is substantial (the air is exchanged in the cabin every other minute), enters at the roof level and travels down to the floor area, where it exits through air vents in the outer walls besides our shoes.
As the air goes back to the air conditioning system in the belly of the aircraft, it passes HEPA (High-Efficiency Particulate Air) filters that catch the rather large COVID-19 viruses. The air is then mixed with new air from the aircraft engine compressors and enters the cabin at the roof level to retake its journey downwards to the outlets sitting at the bottom of the cabin walls.
This orderly airflow will be disturbed by movements in the cabin, and this is why probably the highest risk of contamination is during boarding and deplaning the cabin. The risk during flight is lower, supported by examples given by IATA in the week (see below).
As seen in Figure 1, the mask minimizes the risk of an infected person propagating virus droplets to neighbors in the cabin. Once past the floor outlets, HEPA filters catch the virus. The mask born by neighbor passengers adds additional protection from inhaling any residue aerosol from an infected co-passenger.
Wearing masks
Wearing masks has been part of Asian culture for decades. When I first saw it during travel in Japan, I thought, “people are nervous about getting infected here.” I was wrong. It’s not the persons fearing an infection that wears the mask; it’s the infected person. Asians with flu put on a mask of courtesy to other people.
This is a habit we should adopt, not only in COVID times.
“And we should stop the stupid hand-shake,” says the chief US immunologist Dr. Fauchi. “It has no place in modern society, not now and not after the Pandemic.” This leads us to the touch path.
The touch path
While scientists are clear over the aerosol path, the touch path is intellectually plausible but with a lower probability of infection. How low is not clear as there has been no cases or studies that have proven such an infection chain.
The chain is possible, and the use of an alcoholic gel after touching common areas such as lavatory handles and doorknobs, etc. shall minimize this risk path. The mask, in addition, makes inadvertent touching the sensitive nose and mouth tissues more difficult.
Summary
IATA (the association of the world’s airlines) issued recommendations in the week ahead of a re-starting of flying. Masks for passengers and crew are imperative, and we understand why.
IATA also points to none of the known flights, where post-flight confirmed COVID-19 infected passengers traveled, resulting in infected co-passengers. There were three cases of a passenger to crew infections however, as here, the communication is face to face. Once again, mask-wearing makes sense (this was before crews and passengers wore masks).
We have asked Airbus and Boeing to support us in explaining the in-cabin airflow better, and we will dig deeper into this in the next Corner.
We had a case here of father and son who travelled from US, 9 hr plus flight, and realised they were infected after arrival. The unusual part was the genetic analysis showed they didn’t infect each other.
The airplane issue isn’t so much a little bit of infection to passengers from travelling but the moving infected people around the country. Remember this virus would have started from a single virus moving from a bat ‘somewhere’ and we know air travel spread it quickly around the whole world in 3 months. And it will happen again.
This particular case may not hold up in the long run. Scott Gottlieb mentioned on Twitter in April 24 regarding another study, where 30% of infections occurred inside public transport. When the Japanese tour bus guide got infected way back in February I immediately knew that public transport would be a major transmission vector.
However I do agree about your assertion regarding moving infected people around the country. This threat will mean closed borders for many more months to come.
I would think any form of public transport where many people are compelled into close proximity was a high transmission risk whether trains, buses or planes. During the Spanish Flu pandemic of 1918 most countries would not allow one on public transport without a mask. Given the IATA statement Björns cites of very few if any infections on aircraft and others saying 30% from public transport I suspect it is the frequent movement from embarkation and disembarkation on a urban bus that causes the risk as well as frequent gripping of handles..
Driving an automobile is now the safest form of transport and if I drive from Sydney to Melbourne I’m no more likely to expose myself or transmit an infection than driving from a suburb to the office. I don’t think the problem is travelling distance.
I’m a very carefull person, I wear a medical mask, I keep social distance of 1.5m, I have a small bottle of hand sanitiser on a Karabiner of my belt loop I can quickly use if I’ve had to touch something, spectacles probably protect a little. I carry an mildly antiseptic surface cleaner and use it on the office door knobs and toilet, I figure I protect others as well as myself.
What I’m disappointed with in the western response in most western countries is the almost complete lack of public hygiene education and indoctrination outside of hand washing. Lockdowns are not needed, strict hygiene can be as effective and is nowhere as imposing as locking down and destroying and economy. I would say even restaurants can be open so long as density is moderate and masks are worn except when seated and eating.
The lack of fever screening via infrared thermography is also puzzling. Here is something that works.
Cellphone Geo tracking such as the COVIDsafe app developed by the Australian government is one way people who have been exposed can be rapidly tracked. I would think that having one could become a temporary proviso for entering a restaurant or flying as a passenger. Anyone exposed to an infected person can rapidly be notified, tested and quarantined. It’s better than lockdown.
Geo tracking ( 20..30m proximity ) is more or less useless ( and a privacy nightmare, but the perfect thing to make control fetishists aka conservative politicians really drool.)
Even Bluetooth ( 5..15m proximity ) meshing isn’t selective enough afaics.
Looking at the “Hotspot” ( apre ski, carnival, “fan soaked” events) cases you need close proximity and not just in passing.
Agreed, except that the left wing politicians really drool over tracking and censorship than the conservatives. It is has been left/liberal corporate media, progressives and left wing politicians that have pushed censorship and their “community standard’ and “social norms” and “autoreactive sources” far more so than the faux conservatives we see running most things.
At the very least you would get an alert that you were in the same building or bus (if your silly or have no alternative) at the same time as an infected person and that would trigger you to get tested.
William you should look at who has imfluence on your purported “lefty media” (ownership, advertising placement). IMHO you don’t understand the landscape there.
The 30% infection rate coming from public transport figure comes from 3 separate studies in Taiwan, Korea and Singapore post COVID-19 which all confirm each other. The most likely place to become infected is where you sleep ie a family member, flat mate, fellow retirement home dweller. The public transport spread could be controlled by imposing mask wearing and observing people hand sanitise before they embark but compliance would be hard to ensure.
Kim Iverson does a good job of explaining these.
https://youtu.be/E2EiyUDRNaI
https://youtu.be/hsCo8w67FhE
Transmission vectors in buses and subways appear to be much greater than aircraft using HEPA-level filtering.
That’s interesting but I think there’s a first to that study. The issue is with aerosol particles in the 0.1 to 10 microns, not above in size. These stay longer in the air. And particularly annoying are the one around 0.3 micron. These are a special case which tend to easily go through filters and known as the most penetrating particular sizes. I suggest you ask for a middling of these. The result may be different. 🙂
Long term comparison studies have been conducted amongst thousands of nurses working in hospitals wearing either medical masks or N95 and there was no statistically valid difference despite the lower effectiveness of the medical masks. The infection rate for N95 was 8.2% versus 7.8 % for medical masks. These infections likely were caused not by mask failure but mistakes in touching and handling outside of mask type. I would wear an N95 mask if exposed to dust at work whether building, mining, civil, maintenance, cutting tiles etc. I regret not keeping one handy when working. Some N95 masks have a one way valve to make exhaling easier and stop condensation fogging ones spectacles. I remember a colleague dribbling about a teaspoon of condensate from out of the mask on to my wrist as he leaned to one side of me, so may have some issues there. However even a scarf around the nose and face would likely be quite effective. If one has a serious issue then a P100 mask should be worn. For boarding a plane a medical mask should be enough.
Bjorn,
Would you know if TSA is permitting hand sanitizers to be carried by passengers with their hand baggage into the cabin to use for hand and surface cleaning?
What is the “liquid” limit in milliliters that was allowed?
@Kant: TSA is allowing sanitizer. Articles report 12 oz. You should be able to go to tsa.gov for information.
Thanks Scott. I found out that the limit is 100 ml (3.4 oz) bottles for carry on into the cabin, which must fit in one transparent zip-lock bag 20 cm x 20 cm. Larger bottles you mentioned can only go into checked luggage and so of no help to sanitize anything in the cabin.
I am stuck in Japan with the government’s emergency declaration extended to the end of May. So “Work from apartment” policy in effect and entry from abroad (US, Europe) to Japan is prohibited. So there are no flights to go back, even if one dares to take a chance with covid-19. I do have a ticket to fly from Osaka to San Fransisco on United but no flights. Don’t know when international flights will resume. Till then stuck in Kyoto University!
According to some communications from Airbus and some of it’s air filtering systems suppliers, cabin air seems to be recycled every 3 to 6min (depending A/C type) rather “every other minute).
I have seen 20 times an hour in a report today. I will correct this once we have had more detailed discussions with Airbus and Boeing.
I would have assumed that thinner air and less humidity means less friction to slow breathe/cough thus enhancing potential propagation distance.
Would the simulation results radically change? I don’t know at all but would be eager to!
Humidity level is also known to affect flu transmission: according to CDC researchs, small flu particles tend to hang in the air for a longer time when humidity lowers.
Knowledge about Covid-19 behavior is not advanced enough for a statement but, according to preliminary research, high humidity reduces it’s propagation as well.
There is a study (Fears, et al.) on infectivity of Sarscov2 in aerosols which i dicates that temperature and humidity do not really effect the longevity of the virus. However, Immunologists have long claimed that RH between 40-60% is best to protect the respiratory tract from infections. This I see a bigger problem on a plane esp. long distance. Your resp immune system weakens.
The studies of the half life of the virus on surfaces (as opposed to aerosols) decisively show a significant reduction.
It would be interesting to know what hypotheses Florida Atlantic University simulation took for air humidity and density. And how those in airliner cabin would affect the results
In addition, what kind of mask has been considered in the simulation? “Simple” sirurgical mask or more advanced one (FFP2?)
N95 mask. But the key is the diffusion of the cough jet, a cotton mask does this as well. No mask is a catastrophe, let’s agree on that.
Definitely! 🙂
A “professional” mask with exhale valve is an even bigger catastrophe in context of protecting others.
( and wearing a mask is a better source barrier than a sink barrier in most cases.)
The simulation is done for a normal ground case. How would a cabin altitude of 6,000ft and relative humidity around 10% materially change what we see?
I would have assumed that thinner air and less humidity means less friction to slow breathe/cough thus enhancing potential propagation distance.
Would the simulation results radically change? I don’t know at all but would be eager to!
Humidity level is also known to affect flu transmission: according to CDC researchs, small flu particles tend to hang in the air for a longer time when humidity lowers.
Knowledge about Covid-19 behavior is not advanced enough for a statement but, according to preliminary research, high humidity reduces it’s propagation as well.
Humidity kills the virus. Going from Relative Humidity of 20% to 80% at temperature range of 75F to 85F reduces the half life of the virus from 18 hours to 6 hours. Of course 10% RH May be better or worse. We need to test.
Evaporation ( i.e. drying up) is faster. ( water vapor pressure “@ cosy ambient” vs a reduced environmental pressure.) humidity is low to begin with. Active half life on surfaces will be significantly reduced.
I do not believe masks alone will be sufficient to fully contain the virus, because many people don’t wear them correctly, and do impulsive things like touching their masks and then contaminating the seats and armrests.
I would suggest masks + a face shield at a minimum. To ensure the virus gets sufficiently trapped and people don’t touch their masks & faces, a full-face respirator or helmet of some kind, maybe a clear bubble-type helmet worn by astronauts, would be desirable. Sort of like of those vintage Raindome bubble helmets for Braniff cabin crew.
The mask + face shield is implemented for the cabin crew that faces passenger breathing face to face. For passengers, masks shall suffice if we can make sure the airflow in the cabin is set to an optimal downward flow and people don’t move around more than necessary (except to the lavatory if necessary) during the flight.
> if we can make sure the airflow in the cabin is set to an optimal downward
I imagine this will require disabling the individual aim-able air jets some aircraft have. Older ones if I recall.
There are various studies looking into the use of ultraviolet light in air conditioning systems , both in the ducting and even in areas people use that push the air upwards ( UV has to be kept well above eye level)
UV is a known virus killer
Outdoor UV light kills the virus very quickly, reducing its half life from 6 hours to 2 minutes in the same temperature and humidity conditions. See data at 1.1 minutes.
https://youtu.be/hsCo8w67FhE
UV-C is even faster acting, it is normally filtered out by the ozone layer so viri have evolved no resistance. (Also the basis of the 1950s UV blood therapy POTUS alluded to) Manipulating humidity also kills the virus, more humidity is better. I would say UV light sources could activate in aircraft toilets when unoccupied and they could be turned on in aircraft when unoccupied or simply for short periods perhaps when folks wore protective glasses.
If they could incorporate shortwave UV light into the A/C system to help kill the virus, that would be good. They’d have to have it in an area that was somewhat sealed from eye exposure as shortwave UV light is extremely dangerous to the eyes. It might be a selling point for Airlines. We have cleaner air than Hospitals.
Richard,
They already do have cleaner air than hospitals!
@iain
If you are suggesting this level engagement with precautions in an airplane, what kind of level do you suppose it must be logical to enforce elsewhere, one must link in to the other
In the workplace, home, street etc
Enforcement in an airplane, or if you prefer discipline, must be considered very much easier than elsewhere, and your post is very much motivated by enforcement
How is it logical to cut out airtravel from the general context
Plus you are only considering one aspect – Yet already you are so definitive in your assertions?
Why not outline the enforcement scenarios, with fines leading up to confinement into a special seperated ‘isolation’ cabin for repeat offenders, plus jail term on arrival
Efficient discipline would require some sort of permanent track and trace which would allow evaluation of the potential for discipline of each traveler, who would agree to a ticket price sliding scale based on his record of respecting all the new rules
Turn to Life on Mars to elaborate an overall strategy
Do you attach Any idea of cost, of how even to begin to evaluate cost, to your proposals, or is this not relevant?
Like this?
https://www.blazingcatfur.ca/wp-content/uploads/2020/01/coronavirus-water-bottle-mask.jpg
On top of the recommendations posted here (face mask wearing, etc) I would recommend to adjust the ventilation air gaspers (Personnel Air Oulet) to the closed position. This would minimize the cross contamination from one passenger to the other one sitting side-by-side (even if the infected person is wearing a mask).
Any cleanroom engineer or training manager will tell you it is not possible to teach people to “not touch your face”. That is why cleanrooms went to full heavy PPE for sterile and moonsuits for semiconductor 30 years ago.
That said, the game here is percentages. If my mask reduces my emissions 70% and your mask reduces your intake 30% together we have reduced the chances of transmission 79%. Across the whole population that’s a big gain.
Also note that the COV-SARS—2 virus is pretty large as particles go itself, and tends to be found in much larger water globs. So not hard to filter.
Nicely put and also to be kept in mind, for the ones on the face of the front, its a system. All the parts have to be there.
I thought virus was several orders of magitude smaller than bacteria. HEPA filters catch the most of the bacteria. The N95 masks must be of different technology.
@claes, that is correct. COV-SARS-2 is at least one order of magnitude smaller than the smallest HEPA screen filter opening size. A significant portion of the virus load in the cabin air will not be neutralized using HEPA filters alone.
Here is a report as seen from a passenger. To fly is currently not fun anymore:
https://www.theatlantic.com/politics/archive/2020/05/is-flying-safe-coronavirus/611335/
God I miss bursting through the cloud layer on a typical English day. How could an airline pilot ever suffer from depression?
Having said that, it’s been abnormally clear and sunny since the planes stopped flying.Any data on the effect of the absence of contrails yet?
We saw some the other day and it was, that is the first time in a month!
And they were honking, Winds aloft said anemic but they were pushing 600 mph.
I also noted that star are exceptionally visible at night and birds (and nature in general) much more loud since a month.
Maybe the answer is rather (or also) to be looked for on the side of pollution from industries and transportation (individual cars especially) which dropped dramatically
“it’s been abnormally clear and sunny since the planes stopped flying” If they find that the contrails were decreasing surface temperatures they will never admit it.
Being the Atlantic Monthly this juvenile unnecessarily dour article should be considered creative writing rather than factual.
Aviation will be fun again and must be because it is a motivation for travel. We’ll probably just have to wear masks boarding and disembarking the aircraft when things get back to normal which they must soon. Wearing masks for short periods and being asked to sanitise ones hands is no inconvenience at all. An N95 mask might improve ones survival from smoke inhalation in a take-off crash fire, a P95 (which also removes oil in the air) would be better and a CV95 which has charcoal to move airborne toxins better still. Smoke hoods were rejected because fitting them would cause delays in evacuation the aircraft but a CV95 already worn for hygiene does not have this issue. It can become part of the routine.
A study by Southampton University showed that had action been taken 3 weeks earlier that the spread of the virus would have been reduced by 95%. Even 2 weeks would have stopped 90%.
I find it hypocritical for the Atlantic Monthly to whinge now as back then they were in the camp that undermined the actions that would have prevented the spread of COVID-19: They opposed travel bans, quarantine, went along with a New York politician that told people to attend cinemas and others that said not to wear a mask. That’s the camp they were in. They called those that disagreed with their binary beliefs racist. No apologies have been issued for this uncalled for slur.
In this baffling article they praise the kind of censorship that prevented timely response to the disease:
https://www.theatlantic.com/ideas/archive/2020/04/what-covid-revealed-about-internet/610549/
“In the debate over freedom versus control of the global network, China was largely correct, and the U.S. was wrong.” Do they think that silencing 8 doctors and several Wuhan journalists who warned of the virus in December is largely correct? This Propaganda Magazine is not for decent people. The media more than government was the impediment to timely action.
Then we have the horrific sounding “airborne feacal matter” route.
Research seems to indicate that it’s a good idea to be extra careful or avoid public toilets.
And then there was the speculation the virus could be transmitted by farts.
Old Farts or young ones?
and there was the speculation the virus is sexually transmissible.
In regards to Fauchi, as much as I respect him (highly) , like too many mental types, he does not get the reality to being human.
Of course we are going to shake hands, its built into our culture and its an important form of greeting.
Same as hugging family.
Yes we need to adjust but to damn people for a built in reaction does not help.
We are not Wolverines, we are a social species (some more than others)
I hate shaking hands and would love for that to go away, but I don’t think it’s going anywhere. Handshakes seem too ingrained in certain cultures.
We keep hearing about Cruise Ships and Nursing Homes being dangerous places for catching the COVID-19. We also hear about Church gatherings or other large event’s causing a large breakout of the virus. We also have heard about super spreader carriers and some that never seem to spread the virus. So, how long of an exposure and to what size of a viral load does it take to become infected? I would think grocery store clerks and others interfacing with the public daily would be at a high risk? And I’ve wondered about Flight Attendants in this same category. What I haven’t found is any data on Aircraft crew vs Ship crew becoming infected. Flight Attendant’s are in close contact with passengers for hours a day. Many days a week. Are they getting infected at a higher rate as the ships crew that were on infected ships? The recent USS Theodore Roosevelt Aircraft Carrier that has over 20% of their crew sick with the virus comes to mind. Does anyone have any data on Flight Attendant virus exposure or how many have caught the virus? Does the slight increase in UV exposure in aircraft have any effect on the virus to pilots?
https://jamanetwork.com/journals/jamadermatology/fullarticle/2019958
The ceiling to floor airflow is good from the standpoint of the virus seems to settle on the floor
over time.
https://wwwnc.cdc.gov/eid/article/26/7/20-0885_article
BBC “how long does COVID-19 last on surfaces”
https://www.bbc.com/future/article/20200317-covid-19-how-long-does-the-coronavirus-last-on-surfaces
Behavior of Airborne particles
https://www.cdc.gov/niosh/topics/aerosols/pdfs/Aerosol_101.pdf
I don’t know for airborn crew but French Aircraft Carrier Charles de Gaulle got 70% of it’s crew sick within a month at sea… assumption is that air conditioning system has been the propagation vector.
Assumptions are bad things.
Warships have close contact via the food service areas as well as very close all crew proximity and far more likely that it was that as the long route through air exchange would take out droplets.
Hey Bjorn and Scott – Leeham News and Analysis should make this article free to the public to access, distribute it to news outlets and inform the news aggregators that it is available. Bjorn’s insight and easily understandable explanations will go far in helping the public understand the facts related to commercial flying and assist their decision making. We’re going to need the objective reporting found in this article to help bring air traffic back as quickly as possible.
Bjorn’s Corner are always free.
I would suggest that mankind globsl herd immuity for seasonal flue is quite important and social distancing is counter productive för future, after covud has made it way. Its seems clear that covid will infect most people around the world and there will be a quite high deathtool unfortunately. Its a natural disaster that repeats may one or two times per century and vaccsin seems to take so long time thst the peak have already past when its ready for large scale programs. Mankind should keep flying around globle, socialize and tranfer flue for globak herd immunity against common flue, which covid most likelly will become for years to come.
The issue with the herd immunity theory is that, so far, it is not proven that you are immune once you got it (and hopefully recover without sequelea)…
Coronavirus are not “common” ones like seasonal flu…
You can add in that its pretty hard on the people that die and their families.
Unfortunately its not a volunteer thing, everyone is stuck with it.
We can add in overwhelmed hospitals and short term impact bringing things to an even worse screeching halt (like no food) . While I would be happy to let those daring souls who want to get it, I don’t want to nor do I want to see the world crash.
Its a no brainer to stretch it out over as much time as possible with as few infected at any given times as is possible.
Existing human Coronaviruses(HCoV-229E) cause common colds amoung other respiratory diseases
I agree. Its not a common flue but it might turn to that in future.
My point is thar mankind is effective in creating herd immunities by mobility and social mixing. Art survival strategy? and this should continue post covid 19. Keep on flying….
In sweden, they indicate that perhaps 60% can bee infected and have some immunity hopefully by june in most infected areas. Most people havent even noticed they caught the virus. For elder elder people (+90y) the risk is very high. If bad herd imminity, chance of effective vaccin is less. So we hear from the experts….
The issue with herd immunity is it also culls the herd, it removes the weakest individuals while strengthening the herd overall. One can argue that this is the way of nature, without human intervention.
However in our society, it’s not acceptable to write off the weaker individuals, or knowingly cause their deaths. So better means must be found to protect them if we are to accelerate herd immunity as an intended strategy.
In the long run, we know that herd immunity will dominate. But to accelerate that at the cost of other lives is morally questionable.
As TW pointed out, flattening the infection curve is something we can do that gives vulnerable individuals the best chance. Those chances are enhanced further if we also actively protect them, something which we have largely failed to do.
You could argue that those failures have resulted in almost as many deaths, so the two methods end up being equivalent. But hopefully out of this will come learning about how to handle things better, so that we can allow herd immunity to become established more quickly, with less risk to the compromised population.
Health system is overwhelmed long before herd immunity occurs. Testing for anti bodies is fraught with problems but in NY are they around 12-15% when ‘natural’ herd immunity only kicks at 35-40% ( based on how infectious, measles needs over 90% immunity only achieved by vaccination).
Herd immunity only means there isnt widespread community transmission , not that those who arent immune are ‘safe’ . Do you want the localised outbreak to be your work place, extended family or where you socialise or a hotel you have stayed at.
Herd immunity means that most individuals are immune. That will likely be the final outcome of COVID-19. Vaccination is another and preferable route to achieve herd immunity.
Most individuals do not have a serious illness requiring hospitalization. The vast majority of emergency hospital space that was constructed, went unused.
The main problem, as I mentioned, is that pursuing natural herd immunity as a strategy leaves the vulnerable population at risk. That is unacceptable and must be addressed before it would be viable.
In Sweden, the chief virologist has said the verdict is still out, and he is concerned about this as well, but believes delaying immunity is not the solution either. So Sweden will be a control case from which we all can learn.
The most effective tool seems to be contact tracing, in terms of reducing the infection rate. One key will be if resumption of activity in a non-immune population causes a resurgence. Verdict I still out on that as well.
Herd immunity doesnt mean that at all.
It varies widely for each disease – depending on how infectious it is , that R number again.
Clearly if those with anti bodies are around 35-40% , it means the rest 60-65% are still susceptible in their immediate group , but unlikely if its other clusters in their city.
What you are thinking of is personal immunity from getting a vaccine. I havent yet had the flu one ( its not winter yet) but Ive got the first of 2 pneumonia vaccinations.
Yes, it does. You are referring to the reduction in transmission rates that naturally occur as a consequence of increasing immunity within the herd.
100% immunity is not required to reduce transmission to manageable rates, that’s true. But the issue remains that allowing immunity to develop naturally, through inter-herd contact, puts the weaker members at risk.
That is the whole point here. It’s a concern in Sweden as well, and it’s been acknowledged there. The countering response is, what happens in the long run if you suppress herd immunity by social isolation. Does it just delay the problem, or allow it to recur in future? Or does it suppress the transmission rate permanently? And what are the costs of these solutions, in terms of a shuttered economy and/or lives lost?
it’s not a simple issue, but there are things we can learn, and improve our ability to address it in the future. But not if we deny the issue exists and insist that one or the other is the only solution.
That ends up in an endless argument without learning, like so many other issues today. Defense of being right assumes more importance than acquiring new knowledge and skills. This is the most modern form of stupidity, failure to understand that other views may have merit, and your own view may have flaws.
Rob you keep repeating the same mistake, Herd immunity for covid doesnt mean most are immune at all. Exact numbers arent really known but Sars-CoV-2 is expected to be 35-40% of a population. Thats means the 65% can still catch it. Its not hard to understand that.
Herd immunity is only describes a preventing a continuosly spreading outbreak, not localised clusters , like I said – extended families, work places ( including hospitals), socialising locations,senior living etc. Maybe airplanes with high risk for cabin crew still.
For this virus a herd immunity level just above 1/3 with antibodies ( they only way you can be totally immune, which is how you are confused), the other 2/3 still. have a ordinary chance of being infected
Remember herd immunity is a population effect not individuals
Duke, these are two sides of the same coin. The required level of herd immunity to reduce transmission rate below the critical level is unknown at present, and under study and debate. I have seen estimates reported from Sweden of 60% to 70%. Regardless of the true number, immunity must be established within the herd, at some level. Period.
For the fourth time now, reliance on natural development of herd immunity places vulnerable people at risk. The question is how to address that. You do not address it by telling people who point it out, that they are wrong or misunderstand. Suppression of the idea or discussion or people with those views, does not help, and is not a solution. Why would you even go there?
Additionally we do not know for sure yet the level of immunity that is acquired, or how that plays into the concept of herd immunity.
I never said it’s exactly known , I was giveng a current best estimate.
A good example is at work with an all day seminar with 12 colleagues and an outside facilitator who has Covid but doesn’t know it.
Let’s say 4 of those 12 have anti bodies to give this small group the average of the whole population herd immunity.
Clearly those other 8 are at high risk of getting infected- similar situations have had people infected from holding a book- but because 4 are immune say only 2 of the 8 get infected instead of 3.
Those 2 people’s families and co workers are at further risk.
Thus herd immunity doesn’t mean individual immunity at all, if you don’t have antibodies at all.
Sweden isn’t really relevant , it’s far too soon to have any valid information and any other country try again after 6 months.
Duke, I give up. If your immunity to COVID-19 is anywhere near as strong as your immunity to ideas other than your own, you can rest easy, you’ll be perfectly fine.
Sweden is the only country formally pursuing herd immunity. They are estimating 60% to 70% required to be effective. We know that other diseases are as high as 80% to 90%. They are also estimating 7 undetected infections for every 1 that is known. These numbers make sense in terms of their modeling and how it compares to their actual data. They are also relevant to all countries, as only the chosen path is different, the endgame is the same for everyone,
You claim all this is irrelevant, your own thought process being superior. Good luck with that. In the meantime, the intelligent world is watching Sweden as an early predictor of what is to come, as well as a control case for the relative costs involved.
Herd immunity is poorly understood by most people which is unfortunate because it will mean a lot of unnecessary deaths if they implanted poorly because it requires people to get sick and some will die. The influenza virus has a reproduction rate Ro of 1.3 meaning for very person infected 1.3 more will catch it. When Ro drops below 1.0 the virus will die out. However at a certain point when about
23% (1-1/1.3) of people were infected and immune Ro will drop below 1. Unfortunately SARS-CoV-2 has an Ro of 2.5 in Australia at least so we have to wait for 60% of people to be infected (1-1/2.5).
The way around this is to increase hygiene to get Ro down to flu like levels. This can be as simple as forcing people to wear masks in public spaces such as public transport, shops restaurants (except when seated) and policing that they hand sanitise before entry.
Reminds me of the time years ago when I just settled into my seat and a huge guy behind me made the loudest ACHH_CHOOOOO!!!! I could feel the droplets on the back of my neck and all over my hair. I survived. As soon as I got to my hotel I took a long, hot, soapy shower.
Great comments. From what i have seen I have a lot of faith in aircraft HEPA filtration systems. Although i dont think they are 100% for very small virus particles, but with the gaspers you have a chance at deflecting any sneezing and coughing going on behind you, which I understand can easily project 3 seat rows in front of the offender. However, all of this is a multitude times better than the environment we all have to use to get to and from the airport ie buses, trains and airport buildings, where there there is no filtration nor necessarily much replacement of air and i think that is a real problem. So masks are going to be essential in all aspects of the travel experience. Train and bus manufacturer are also going to have to think of a way filter air and improve air refresh – its not like you can open a window on any recent models..
HEPA is a very old 1940s technology (from aviation, submarines) and has for a long time been supplemented (was supposed to be replaced) by far more effective systems that can handle the finest of pollution, pollens and virus. If you’ve got someone with hay fever a simple $100 HEPA standalone System in the bedroom and living room will make their life much better, as it did mine, without antihistamine drugs but the more advanced professionally systems you would purchase (about $600 a bedroom sized unit) can remove the finest of pollutants, viruses, bacteria moulds. Most also have charcoal filters to remove chemicals that might be gassing of plastics, paints and varnish. If you live in a city you should consider investing to protect your respiratory health. One thing that is noteworthy is that it eliminates the dust buildup in a house saving you on dusting. All of these things concerning air conditioning and ventilation systems have been known for 70 or more years. It takes a tragedy for action and regulations to come in such as when the death of war veterans in an American convention “legionella”caused regulations for disinfection of wet cooling towers. My sisters first job as a biologist was taking samples of microbes on the other side of air conditioning, inside the ducts. They’re full of it unless fitted with filters, but as with most things nothing is done and concerns are rubbished and ignored till a price is paid.
It seems in a case the COVID-19 disease is spread primarily on urban public transport such as trains, trans and buses whereas aircraft are an insignificant contributor. I suspect you are more likely to catch the disease in the terminal during checkin. Aviation has a pr issue.
It seems that moderate action in terms of filters, disinfection, electro static precipitators, face shields for counter staff has a very great effect.
Thats mostly baseless. The worst hit place in Germany is Heinsberg a city of 250k , not the teeming metropolises of Berlin, Hamburg etc
https://www.dw.com/en/load-lifts-on-german-city-hardest-by-covid-19-pandemic/a-53227032
The Heinsberg spread is assumed to have come from a festival in February. This is a bit of an unusual time for a festival in Germany. Being fond of visiting them myself when in Germany they usually go for the weekend. Grandparents may attend during the day sitting with friends in a tent and take a sit down meal with their children and grandchildren, young people meet up and people go to a range of concerts in a beer tent listening to anything from an oompahpah band to modern dance and rock or go to a show. If kids get it they’ll pass it on to parents and grandparents. A small city like Heinsberg will likely have one or two railways stations and a small tram system but the bulk of people will get around by car or push bike. Berlin is not such a large city and the public transport does not seem crowded relative to many cities.
The virus is clearly exceptionally contagious compared to the flu and clearly airborne which is why its transmission reproduction rate is 2.5 versus 1.3. What seems to work is:
1 Keep a distance of 2 meters, this is reasonably effective but still carries risk if exposure is long and people cough or sneeze.
2 Wear a mask. This seems to be highly effective. It prevents spreading to other by the random coughs, sneezes and spluttering’s infecting others and by by diffusing the breath. It also seems effective at protecting the wearers by absorbing course droplets of the virus.
3 Hand cleanliness. A key part of controlling the virus.
4 Ventilation. It seems aircraft ventilation is quite effective at preventing the spread of the disease once people are seated as very few infections can be traced to aircraft due to the high downward circulation of 20 changes an hour.
5 The much poorer ventilation on buses and urban trams and trains seems to be a problem combined with higher densities, the frequent movement and jostling of people and the need to grip hand rails. Failure to wear masks and hand sanitise on entry to the bus and exit is probably the cause in my view.
In Australia the lockdown has taken the reproduction rate of the virus from 2.5 to 0.5 at the cost of economic destruction. At R=2.5 60% of people will become infected before the virus contacts so many immune people it no longer spreads. 60% = (1-1/2.5). Nothing will alter this except by permanently reducing the infection reproduction rate by increased hygiene or rapid detection of carriers and their quarantine. This means Sweden will have no more deaths than any other country, they’ll only come faster. According the Heinsberg study 0.49% of those that become infected will die. If the infection rate can be cut permanently to flu like levels of 1.25 by hygiene then the equation is 20% = (1-1/1.25) and the death rate can be cut by 3. Hygiene will likely also promote the spread of less dangerous strains of the virus that confer immunity.
If you are afraid to catch covid-19 in airplanes, do not travel by air.
Get the point. Ofcource weak individuals should be protected as much as possible and thst have been the aim of the strategy. Eventhough it has extremly difficult to prevent leakage into elder populstion. Another aim is to flattening the curve not to exchaust the capacity. It seems under control in Sweden now. The expected number of desth is uncertain but a recent guess is sround 5k of 10m pop, compsred to 2k in a severe seasonal flue. Most elder elder. The key point is that all persos will receive the virus and the hope is to vaccin or other medicants to suppress the virus to reduce the number of death. Seams as middel east and africa have somewhat higher resistance.
Niklaus, I agree with this assessment and Philby’s below. The question in my mind is how can we respond to these situations n a better way. Hopefully that will emerge in the analyses that will follow.
The equatorial and/or hot and/or humid regions may have a climate effect that alters both the activity level of the virus and social interaction of people carrying it. They have a different pattern of cold and flu viruses as well.
@Rob
In central africa they say they are much tougher immune wise, they also are used to malaria which does kill ‘vulnerable people’, mostly the old
They also live old and young on top of eachother – they say putting the old apart is putting them at risk depriving the group of knowledge and experience, such as how to face and deal with difficult situations, culled from memory of the past
such would have been useful in the north, people live better in groups, clan, or families – in general: to make the exception the rule is a recipe for continuous disasters
the idea and practice of communal life does have advantages over the idea of life as a collection of autonomous individuals
‘protecting the vulnerable’ is composed of many parameters, not merely the contagious or not contagious disease ‘prevention’ – to select this as the one parameter is foolish and self defeating
they also lack the prevalent lifespan extension competitions which provide for such false measures of life
otherwise Rob, on a personal note good to see you back, I was explaining the need for your comments here only the other day
Thanks Gerrard. You raise good points about how the social integration of seniors varies within cultures, as well as differences in the vulnerable population, and how these could be factors with COVID-19. That illustrates really well the complexity of the issue and how much there is yet to learn and understand.
Due to the different climate Africans and Europeans have in past times died of different diseases. For Africans parasites such as tropical disease are a sever problem. Europeans died in the millions from pulmonary and lung diseases, especially the young such as babies before they reached reproductive age (determined by parental nurturing capability) but also the elderly. Malaria which was common in Europe, Germany and Britain was eliminated by ongoing swamp drainage from the 16th century. Cold kills from lung infections, plain cold and starvation but also kills parasites every season. Our social order, the way we live our family is likely effected by this and so likely is the genetics of our immune system, sickle cell percentage etc. There is sometimes nothing to learn since the problems we faced were different.
What is interesting is the range of disease that entered Europe when cities developed and how they were conquered not by immunisation (which didn’t exist) but separation of drinking water from sewage water by civil works, the provision of private as opposed to communal toilets and the widespread availability of running water for cleanliness, the collection of garbage. it seems we need to up our hygiene to account for the large number of objects we are touching eg touch screens, bus hand rails and the ventilation in our public transport and simply the inculcation and imposition of good habits.
i really don’t think many people ‘get it’ when discussing coronavirus.The answer is there if you read carefully and do not let ones natural bias and hopes get in the way.
Covid19 is just one of an enormous family of virus’.There are 4 varieties of the common cold for instance.Some can kill others don’t.It is incredibly difficult to create vaccines for this family.I believe I am right in saying no one has ever achieved it with any member of the family (100% immunity).Been trying for over 60 years.They might make one that has an x% of immunity like flu jab (40%) and a new one required every year.
Many scientists think the best we can hope for is a vaccine that reduces the effects of CV19 thus making less deadly.
Timing? Very very unlikely to be 18 months.Dont take my word for it read for yourself.2-4 years more likely.
Soooo
Just about Everybody will eventually catch it.This is the Swedish model if you like.But
Under 25,s get it so mildly that they are effectively immune.
25-65 will not get very ill unless they have additional underlying medical issues.Think flu.
70-80 yo need to be very careful indeed.
Over 80 seems like a 40% chance of dying.
Who should fly?
Think the answer is in the numbers frankly.
The reason cold viruses dont have vaccines is the rate of change is too high to have a useful vaccine even for one year. Influenza changes at a slower rate , enough to have yearly vaccines, Sars-CoV-2 changes at a slower rate than flu so maybe a 5 yr vaccine might be possible.
In addition there is a lot of work looking at a prophylactic agent, which isnt a vaccine as such but if given to healthy people can assist in prevention of a disease. This would be very useful for those working in healthcare and public facing roles such as cabin crew. Anti biotics are sometimes given in this role after surgery, dental procedures etc
An N95 Mask with an exhaust port is NOT the way to go. That is exactly what to filter, so a plain N95 mast is better.
Use disinfectant by injection or hit your body with strong UV light. Take a bleach shower.
UV light can be used in ventilation ducts, toilets etc on aircraft. Ultraviolet Blood therapy was in use in the 1950s. The blood is taken out of the body, subjected to UV, and returned. It fell into disuse as more powerful antibiotics became available but the Russians and East Germans used it and developed it well into the 90s. There is also PAD or Photo Activated Disinfection which is often used to treat gingivitis, root canals and nasal decolonisation. When used to decolonise the nose it reduces post operative infection rates by 85%. It is being investigated for use in combating COVID-19 because it seems to stop the spread of corona virus into the lower respiratory tract. Ayto Bioscience of Colorado has developed an ultraviolet system that can get inside the body via the lungs via a respirator and LED and attack the corona virus. The president was speaking to William Bryan from homeland security asking the kind of questions an ordinary person would ask and obviously misspoke because of the wide range of treatments being investigated. He never mentioned bleach. The moron media added layers of distortion. There is also photoactivated medication which gets interesting if the medication can be attached to an antigen which then attaches to the virus and can be activated by UV.
Good response Dukeofearl.All correct.But many people think Flu vaccines simply work.On average they have a 40% effective rate sometimes higher sometimes useless due to mutation.
Clearly you know this stuff but so many are hoping on a miracle that may never come.
Your second part was right on the money.What we can perhaps hope for are developments that can reduce the power of the virus so it becomes less deadly for the older population,
However I fear we may need to recognise that CV19 is now endemic and we will have to live and work with it -as we do with many other infections.
Suggest LeeHamNews having a poll of who would fly at this time. I might fly if the middle seats are left empty on narrow bodies. On five across seating, the middle seat and one seat on the double side. Also, I would like to see a plastic polypropylene curtain between rows. This would have to be Federally mandated and I’ve seen flight attendant unions looking for something like this. This situation could be with us quite awhile.
Instead of putting plastic shields up everywhere, why not produce a plastic helmet with a HEPA filter to breath through? Sort of a don’t raise the bridge, but, lower the river option. I think it could be done for maybe $250 per person? It might look funny, everyone walking around like Spacemen, but, it should cut the virus transmission to the human body by a large percent, if folks followed the proper procedures for putting them on and off. (wash hands, wash helmet, wash hands, take off helmet etc) Then, you could then open up things a lot more, with less risk.
https://www.cdc.gov/niosh/npptl/topics/respirators/factsheets/images/paprimg1.jpg
Yes, that would be even better. The concern would be the sanitizing between flights. I wouldn’t mind looking like an astronaut. Small trade to fly and not be breathing other people’s germs.
Aerosols do spread even when you cough wearing an N95 mask. The force of a cough is sufficient to cause aerosols to spread in a different pattern rather than directly outward. Most HVAC experts will say, at most, that HVAC systems reduce the viral load but none will say it’s eliminated. A recent NAS study concluded that coughing passengers with covid-19 can be quite infectious to neighboring passengers. As passengers get up and travel in the cabin, there is even greater opportunity for infection and spread. I wish the airline industry had done these studies, so there’s a lot of conjecture here.
Most passengers are not wearing N95. Some are wearing loose bandanas, scarfs, etc. Even ordinary surgical mask aren’t very effective for anything but large droplets. These coverings might be OK for reducing Rt in common casual settings but not inside aircraft and airports for many hours.
You suggest covid-19 aerosol recirculation within the HVAC system is of little concern. This may be an over-simplification or plain wrong. Covid-19 virus particles are known to remain viable in the air for a considerable period. Covid-19 is .12 micron. A not-insignificant fraction of droplets from a cough will be below 0.3 micron. The best “hospital grade” HEPA filters will not filter out less than .3 microns. Only systems designed for clean rooms can get down to .1 micron. When the filter accumulates virus it may start passing them as the droplets evaporate. This calls for good simulation studies, not conjecture.
There are lots of unknowns. Are your reassurances are based on actual studies of plane HVAC systems? If they are, I would greatly appreciate this information!
HEPA Filters on planes are not effective against Coronavirus, the diameter of these corona viruses are smaller than 0.1 µm, and HEPA Filters cannot reach this, so this is bad science being marketed by Boeing and Airbus and the airlines…
There are many scientific studies and even graphs depicting the ranges of things… scroll to bottom of this page link and see the graphical representation and realize than the big scam going on…. HEPA Filters are not able to touch this region.
https://www.respilon.com/coronavirus/english/respipro-respimask-r-shield/