Leeham News and Analysis
There's more to real news than a news release.
 Leeham News and Analysis
Leeham News and Analysis
- Dissecting Boeing CEO’s statement next new airplane will cost $50bn April 15, 2024
- Bjorn’s Corner: New engine development. Part 3. Propulsive efficiency April 12, 2024
- A350-1000 or 777-9? Part 2 April 11, 2024
- Pontifications: Boeing “transparency”–not so much. April 9, 2024
- Airbus charges and write-offs since 1999: more than €33bn April 8, 2024
HOTR: Don’t get over-optimistic on COVID-19 vaccine news
By the Leeham News team
Nov. 10, 2020, © Leeham News: Pfizer yesterday announced it’s on track to produce a COVID-19 vaccine that appears to be 90% effective in trials. The company is one of the world’s leading drug makers.
This is good news.
 But before jumping to the old cliché about a light at the end of the tunnel, LNA’s Judson Rollins cautions, do the math.
But before jumping to the old cliché about a light at the end of the tunnel, LNA’s Judson Rollins cautions, do the math.
“Read the fine print at the end of the press release,” Rollins says.
“Based on current projections, we expect to produce globally up to 50m vaccine doses in 2020 and up to 1.3b doses in 2021,” the press release says.
“It’s a two-dose vaccine, so divide by two to figure the number of people who could be immunized,” Rollins says. “Even if a second candidate is approved and can be produced in the same quantity next year, that means just 17% of the world’s population will be vaccinated. And that assumes everything goes according to plan.”
Rollins did an extensive analysis of how quickly global air traffic would return to normal. In his July 13 post, Rollins projected that traffic won’t fully recover until 2024 at the earliest or 2028 at the latest. It all depends on how quickly a vaccine was developed, how quickly it could be distributed globally and how quickly people had confidence in it.
“We’re in only the second or maybe third inning of a very long ball game,” Rollins says. “Vaccines kill off a virus by denying it bodies in which to reproduce. If you don’t innoculate enough of the population while immunity lasts, you’re back to square one.”
Main deck freighter demand
There was one notable exception to the soaring wave in aviation-related stock prices after the Pfizer announcement. “Stunningly, Atlas Air stock fell 14% on expectations that [passenger aircraft] belly capacity is coming back and will supplant freighter demand,” Rollins added. “Did investors forget that freighters will be needed to transport all those refrigerated vaccines?”
MAX recertification
The Federal Aviation Administration appears ready to recertify the Boeing 737 MAX as soon as next week—Nov. 18, in fact, Reuters reported yesterday.
The MAX was grounded globally March 10-13, 2019 following the fatal crashes of two 8 MAXes, in October 2018 and March 2019. Three hundred forty-six people died in the two accidents. Europe’s EASA previously said it expects to recertify the plane later this month. Transport Canada and Brazil’s regulator—rounding out the Big Four in the recertification process—haven’t said when they may act.
China’s CAAC was the first regulator to ground the MAX. The agency has been mum on its plans. But with China, politics often trumps everything. A trade war with the Trump Administration may influence China’s actions.
Morgan Stanley caution
Meanwhile, Morgan Stanley yesterday cautioned that Boeing could lose more orders for the MAX. An analysis notes that 29% of the MAX orders are common with Airbus A320 family customers. If, because of COVID, there is an oversupply with customers, Morgan Stanley believes Boeing could be hit with cancelations rather than Airbus.
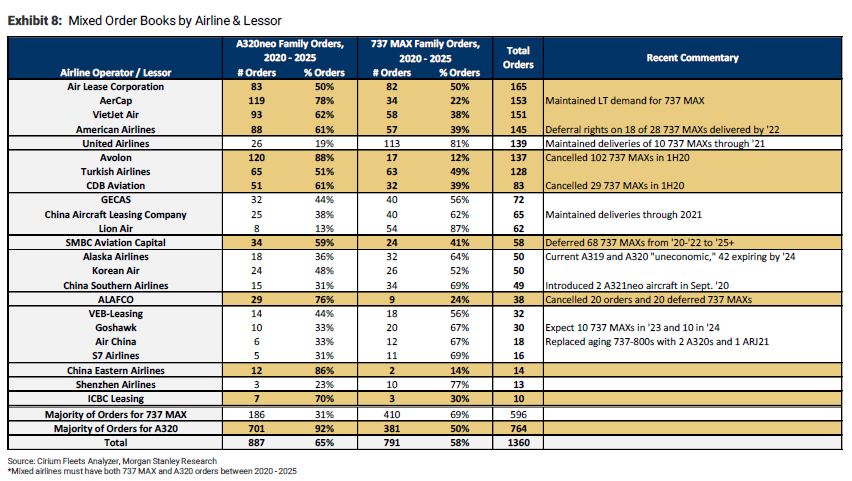
This is because scores if not hundreds of MAX orders are now delayed by 12 months or more. Twelve months is when most orders may be canceled without penalty.
However, LNA previously noted that this is typically on a rolling basis—not for an entire order.
We do not need to vaccine everyone. Increasing number of people already had it. JHU gives currently 50 Million positive tests, it is safe to multiply this by factor of 10. Worldwide the really risky people live in the Western hemisphere and some parts of Asia (old, obese, diabetes).
Globally there are 9% of the population over 65.
Hence, it is likely that even with a limited vaccination the mortality can be reduced by an order of magnitude, at which point it actually is in the same ballpark as the flu (a bad one though). Some parts of the world with much younger population have not seen Western mortality rates (which are currently estimated at 0.8% of all infections (not just the registered cases)).
So, I see an increasing chance that traffic will pick up, although surely not 2019 levels.
I think your general analysis is very well reasoned.
However, as regards “bubble” countries like China, Taiwan, Singapore, Australia and NZ, one can imagine that they won’t be allowing anybody in who hasn’t been vaccinated. Of course, one can ask oneself how long they’ll be able to maintain such an approach.
As a Citizen of NZ, our economy is recovering very well whilst maintaining the bubble. We are in the process of extending the bubble to the Cook Islands, and during the next 12 months will continue extending that. When we have effective Covid vaccines travel will open up. As a frequent traveller I am totally frustrated by having to cancel this years cruise. BUT I am a 75 year old alive and well. Our Government was re-elected on a landslide because of the strong stance on Covid. Trade is fine. The main issue is shortage of shipping for the volumes sold! My gut feeling is travel will start returning in 2022. I suspect, like the ‘flu, Covid will need annual shots as it changes. I do not believe anyone who has had it will be immune long term.
Interestingly enough: we have an election coming up in NL next year, and the main party in the present coalition is also enjoying strong support due to its (totally different) stance on CoViD. The same applies to the government in Sweden.
I agree with your opinion that nobody will be immune long term — either via infection or vaccination. It remains to be seen, however, to what extent the currently proposed vaccines offer any meaningful immunity to people over 65. If they don’t, then the only way to protect seniors will be via continued sequestration (obviously undesirable) or some degree of transient herd immunity in the population under 65 (not entirely reliable, at best). Or, those that aren’t too old/vulnerable will just have to bite the bullet and take their chances.
If it’s any comfort to you, seniors in NL that aren’t in care homes are just going about their normal business, within the bounds of the current set of socialization rules. I live near a park and see several of them out and about every, without masks (not required or even recommended in outdoor spaces in NL). There are special “senior hours” at supermarkets for those who are crowd-shy under the present circumstances, but many just elect to go during normal hours.
Like you, I’m a frequent traveler, and am annoyed by the currently impaired travel possibilities. What makes the situation worse is that, with a little bit of creative thinking, travel restrictions could be greatly relaxed. But that seems to be a bridge too far at present.
Wile this is not deeply technical I believe its a good summation of the status and worth listening to.
https://fivethirtyeight.com/videos/what-to-make-of-pfizers-big-vaccine-announcement/?cid=rrfeaturedvideo
I would not be able to follow the in depth data details, that kind of statistical unraveling is no where near in my wheelhouse.
This as well as the site that Rob lists further down are good as they provide the summation needed, both for the good part and the unknown parts.
Interesting digging into death rate in Sweden, which apparently did not handle care residences well initially.
https://www.aier.org/article/swedens-high-covid-death-rates-among-the-nordics-dry-tinder-and-other-important-factors/
(Whereas Florida did, grasped what happened in Italy and acted quickly and assertively for care residences, starting with ones that were not great in last inspection.
Florida was also tough on hospital-care residence interaction, ultimately setting up temporary facilities such as in motels so hospital could discharge customer without dumping them back into their care residence.
(Sweden did not do much of a lockdown, has more respect for individual rights and the benefits of productivity than most fiefdoms.)
Elsewhere, collateral damage is rampant. http://www.moralindividualism.com
The mortality is just ONE of the problems of the virus and looks like the natural immunity is not for ever (back to square one every year?)
There’s absolutely no reason to believe at this juncture that a vaccine will give long immunity either: figures of “about 6-8 months” are often cited.
This claim is false, there has been research to suggest that immunity may linger, and also there is no evidence yet in the general population of loss of immunity. The consensus of the medical community is that there is cause for hope.
It might be more truthful to say that we don’t know for sure yet, because there has not been sufficient elapsed time or experience with the virus. But the signs currently point to longer immunity, rather than shorter.
“there is no evidence yet in the general population of loss of immunity.”
INCORRECT
https://www.pennlive.com/nation-world/2020/10/evidence-of-diminished-antibody-immunity-to-covid-19-over-time-a-uk-study-reveals.html
Amusing that you categorically state that someone else’s assertion is wrong, when you yourself make a wrong assertion, and also try to rely upon vague and nondescript syntax such as “MAY linger” and “cause for HOPE” to make an objective point. I know you desperately need to put the whole vaccine subject into a neat, labeled box, but others aren’t constrained by that urge.
Rob is correct on this one.
There are only 365 days in a year. We can only know a vaccine has been tested day 180 and can say its known to be effective for 6 months.
That does not mean at day 181 it quit. At day 190 it might (in some) but what we need is how long it last in most and what the percentages are.
Rather than idle speculation based on no facts, we need to see what the data says.
It will be reviewed and we will have a spot indicator.
Like votes, more information will come in as time goes by.
Pennsylvania at one time was solid for Trump, that did not last, votes were counted that had been mailed or drop boxed and it changed (and they knew it would but you can’t just guess at how much, you have to count the vote, ie get facts)
In fact Trump never lead, the count was biased to same day ballots.
He in fact was behind all along, the data had not been compiled yet.
Let the data get compiled.
Bryce, this is an example of the “outlier science” I mentioned. Yes, this study shows that the falloff in the first responder antibodies is real. That is not inconsistent with what I’ve said, nor is it evidence that immunity is not possible or not present.
It looks at only one aspect of immunity. Other studies have looked at T-cell responses and the presence of other antibody types in bone marrow, which do indicate they have remained for the duration we are able to measure at present. As time goes on, these results can be tested further.
You keep referring to the same studies because they reinforce the conclusions you’ve already reached. But if you broaden the scope to include all the research, you may reach a different conclusion, or at a minimum, leave your conclusion open. Note that you are the one that said there is no contrary evidence for immunity, and that statement as I indicated, is completely false.
We also don’t see the lack of immunity in the general population, in terms of re-infections. That is not “INCORRECT” as you claim, that is an absolute fact.
And we know that the medical community is optimistic about the vaccine, there would be no point in pursuing it if the longevity prospects were hopeless. So that is the message that should be put forward, unless and until the trial data show otherwise. They do not, at present.
@TW
Seeing as there’s essentially no broad evidence on longevity *at all*, my statement above is not incorrect…particularly seeing as it was in response to JD Evora’s “for ever” remark. The only *evidence* we currently have is what was published yesterday — which only told us that, after a period of two months, it appears that 10% of vaccinees can nevertheless get infected. Although there might be “hopes” or “indications” of a particular immunity longevity, that doesn’t constitute “evidence”.
I know that Rob is very loose with his terminology, but surely you’re not going down that road also?
This is again false. The evidence for immunity does exist, though you choose not to acknowledge it. It cannot be certain or even known at this time, how long immunity will last. But that is not a reason to deny the potential of the vaccine, within any rational frame of reference.
Bryce: While Rob is selective in his views (if a businessman says it it must be true)
factually for a vaccine we don’t know past what we have time line wise.
I separate my hopes (high) out from right now we don’t know if may be a bust, it may be in between or it may be a major success.
Two trails were halted (maybe 3 now) while they looked at details of why someone got sick or died.
That is normal, people do get sick and they die for all sorts of reasons and you need to sort out if it was something else or Vaccine related.
All I am saying is why speculate when the end of the trial people who are experts in this will suss out the data.
Then we can make some determination individually how we feel about the details.
Personally if its a discomfort thing vs catching that damned stuff I will take the discomfort.
And long term if its effective we still don’t know how the population will react as the issue has been tainted by politics (though we made a huge step up to go back to science).
And that does not mean there is no risk, there is always risk. Getting in your car and traveling is a risk.
Lets let the data come in.
they can speculate all they want if it is and what the dates of recovery are, shoot, I can do that and not charge them anything for it.
They don’t know any more than any of us do. This is a new one off and its just blithering.
@ Rob
There we go again.
If this “evidence” does indeed exist, then why can’t you provide us with a link in which it is elucidated? You dodged the same question yesterday.
And then you accuse others of “outlier science”.
Bryce, my expectation is you would do your own independent research of this, as I do. But here is a relevant Google search, take your pick of the results:
https://www.google.com/search?&q=coronavirus+immunity+t+cells&oq=covid+immunity+t-cells
Here is one of the most recent, but only one of many to arrive at the conclusion that antibody measurements do not provide a full picture
https://www.reuters.com/article/us-health-coronavirus-britain-tcell/english-study-suggests-t-cells-could-be-sufficient-to-protect-from-covid-19-idUSKBN27Q004
@Rob
There’s nothing in your listings relating to the longevity of a *vaccine*.
There’s also nothing indicating longevity of immune response longer than 8 months.
My comment above, which started this sub-thread, said (emphasis added):
“There’s absolutely no reason to believe at this juncture that a *vaccine* will give long immunity either: figures of “about *6-8 months*” are often cited.”
To which you responded: “This claim is false”.
Your inability to read is alarming.
Bryce, 8 months is about the boundary of what we can positively say right now, given that is the duration of the pandemic in the West. But as TW pointed out, there is not reason to believe that the immunity will magically end tomorrow. In fact there is reason to believe that it won’t, based on results from China from an additional 3 months of history.
So we are going on 11 months with their results, pretty close to a year, which is as far as anyone has predicted at this point, but does not represent a hard limit.
Also there are among the search results I gave, reports that point to T-cell response produced by the vaccine.
https://www.fiercebiotech.com/biotech/pfizer-reports-strong-t-cell-response-to-covid-19-vaccine
You can deny this all you wish, denial is a safe haven for those who have already drawn their conclusions. If the science contradicts these views, or the trial results soon to be published do, I will gladly reverse my position. But for now, I’m going with the evidence, and will counter anyone who tries to deny it to others.
Reality is we simply do not know.
Relatively few people have gotten re-infected (and I understand Covd itself is not the same as Vaccine)
Measles is life time, polio is life time – others need a booster.
Just call it unknown right now.
I had that discussion with a mfg over a new type compressor and while I needed the data, they sim,ply said, we have run it for 10,000 hours and that is all the time till now. Give us a year and we can tell you 18,000 hours. Its going to take 3 years to get a solid data on how long it lasts.
Ok, I get it. We are 10 months into this more or less and far less with a vaccine.
Month by month we will get more data.
I got the measles before the vaccine, it was an ugly and awful 5 days let alone the health risk.
I count myself fortunate that Polio vaccine came out and no one in my family got it.
The fact that we have 94% tentatively effective vs the 70% they hope for is a hopeful indicator.
I am not hanging my hat on it. But if it passes the analysis as safe I am first in line for it (well behind the first responders)
So maybe after 10 months it needs a booster, or its an annual like the flu shot, yipeee!
None of us wants to see family affected by this and too many have.
Too bad Jack Dorsey can’t weigh in here to settle what the truth is here. I always like Tech Overlords to tell me what to think.
@Martin Z
One point you might like to consider is that T-cells don’t prevent infection…they merely combat infected cells, thus reducing the severity of illness associated with infection. If you want to *prevent* infection, then you need a sufficient antibody titer. That convolutes the concept of “immunity”. Importantly, when antibody levels become too low, a person can potentially still carry and transmit the virus despite functioning T-cells; such a person can still be a menace to his environment…which is an important point in the current context.
Let us know if Jack can throw any further light on the matter 🙂
Others will now (doubtless) weigh in to say that this is rubbish, because it’s not cheery enough for them, and doesn’t sit well with their desire for the pandemic to just go away 😉
Bryce, the science on this speaks for itself:
https://www.cebm.net/covid-19/what-is-the-role-of-t-cells-in-covid-19-infection-why-immunity-is-about-more-than-antibodies/
“Studies assessing the clinical features of patients infected with SARS-CoV-2 have reported an incubation time of 4 to 7 days before the onset of symptoms, and a further 7 to 10 days before progression to severe disease.
For many primary virus infections, it typically takes 7 to 10 days to prime and expand adaptive T cell immune responses to control the virus, and this correlates with the typical time it takes for patients with COVID-19 either to recover or to develop severe illness. This raises the possibility that a poor initial T cell response contributes to persistence and severity of SARS-CoV-2, whereas early strong T cell responses may be protective.”
“Potential for Long-Term Immunity”
“Early research suggests that the antibodies in people infected with SARS-CoV-2 dropped significantly within 2 to 3 months, causing concern that humoral immunity against the virus may decline rapidly. However, it is a normal part of the immune response that antibody levels fall after an infection has resolved.
For example, in seasonal coronavirus infections, antibodies start to decline at about a week after infection and typically only last for about a year. It should also be noted that memory T and B cells are formed after infection; these can be reactivated when another infection with the same virus occurs and could provide long-lasting immunity.
A preliminary study that has not yet undergone peer review has shown that memory T and B cells were found in patients with mild COVID-19 symptoms who had recovered and that these cells persisted, suggesting the potential for longer-term immunity.”
“SARS-CoV-2-specific memory T cells have also been detected in exposed seronegative healthy individuals (relatives of confirmed cases), which may indicate asymptomatic infection. One study has shown that ~93% of “exposed asymptomatic” individuals had a T cell response to SARS-CoV-2, despite seropositivity in only 60% of cases.
Asymptomatic infections may therefore be more common, and antibody testing alone may underestimate the true prevalence of the infection or population immunity. SARS-CoV-2-specific T cells were found in most of the convalescent patients in this study, which is a promising sign that infection may give rise to immunity.”
Excellent points thankyou.
There’s ‘herd immunity’ too, IIRC guestimates months ago were a threshold of 60-70%, whereas the bad type of measles is 80% (a well known disease of course). Perversely ‘lockdowns’ delay reaching herd immunity.
On top of this data regarding availability of the vaccine, there’s also the question of uptake. Although the manufacturers generically classify the documented side effects so far as “mild to moderate”, we do have more details of those side effects — which include significant fever, shivers and fatigue, usually passing off within a day. However, upon closer inspection, the magnitude of these effects is not to be taken lightly: one subject woke up in the middle of the night (after his second dose) with shivers that were severe enough to cause him to break a tooth, and fevers of 104 F / 40 C were not uncommon. Fevers like this are usually a no-no when it comes to vaccine approval for broad use. There are certainly plenty of underlying medical conditions that would act as a contraindication when considering use of this vaccine.
https://www.cnbc.com/2020/10/01/coronavirus-vaccine-trial-participants-exhaustion-fever-headaches.html
Moreover: remember that pregnant, pre-natal and post-natal women have still not been cleared in any vaccine trial, thereby excluding (short-term) applicability of this vaccine to anyone in that group. So, where this vaccine is concerned, families planning on traveling with young aspirant mothers won’t be getting on planes any time soon.
The clinical trials permit members to post their experiences on-line, as long as they do so anonymously. They don’t know if they have received the placebo or the vaccine.
Many reported irritation and rash at the injection site, as well as a brief illness (24 to 48 hours). That’s to be expected and is similar to the flu vaccine. Although the vaccine doesn’t give you COVID, it does trigger an inflammatory response in the body. Remember that’s basically how it works. How severe depends on the individual.
There is always a range of reactions to a vaccine, and the detailed results will evaluate that. The trial members are given an app to log their experience, and which also provides instant access to a doctor. For the majority of cases, that was sufficient, the person did not require medical care after injection.
Uptake rate will not be a major issue initially, as dosages will be limited to the vulnerable at first. It could become an issue next year if the general response to the vaccine is negative. If the efficacy remains high (80% to 90%) at the end of the trial, and within the first vulnerable groups, people will have greater confidence. If the efficacy is at the minimum 50%, some may choose to forgo and take the risk.
Judson’s point about longevity is valid, many decisions will depend on how long the protection lasts. But if the efficacy remains high, that mainly extends the time required for general vaccination.
“Uptake rate will not be a major issue initially, as dosages will be limited to the vulnerable at first”.
Great that you have a crystal ball to be able to see all this! The rest of us just have to content ourselves with reasoned opinions rather than proclamations Ex Cathedra.
As regards the vulnerable: I can very much imagine that GPs will be reticent about subjecting frail old ladies to the risk of a 104F fever and teeth-breaking shivers. So we’ll just have to see how this pans out. Particularly if it transpires that efficacy is low for elderly recipients (information that was not released yesterday) and/or that longevity of protection is sub-optimal.
Also, since aviation is the context of this website, uptake among the general population is of critical importance. Airlines are not going to be saved by masses of vaccinated vulnerable old ladies who want to get on a plane.
Bryce:
I got a pneumonia shot. My arm hurt like the devil itself for 3 days after.
I will take that over Pneumonia.
@TW:
I got duodenal IBD as a side effect of using a relatively “safe” medicament a few years ago. It lasted 3 years, and I was lucky that it eventually completely disappeared. With that experience behind me, I can *very* much assure you that I won’t be taking the medicament in question ever again…regardless of the severity of the condition that it is intended to treat.
I’m glad for you that you only got a sore arm from your pneumonia vaccine. I also only got a sore arm from a DPT vaccine a few years ago. But those vaccines weren’t rushed, whereas the current CoViD vaccines are.
This is a matter of personal choice. I’ve had CoViD, and I know 10 other people who’ve had it. It’s not the Black Death — unless you happen to be in a very particular niche group of the population. If you’re in that group, feel free to take the vaccine. I will exercise my right not to do so until I have *much* more data.
Bryce, this is absolutely correct, you have the right to refuse the vaccine based on your experience, values, and beliefs. No one is disputing that.
But so do others have that same right, and also the right be to be provided with full and truthful data, information, and evidence, so as to make their own decisions.
This is where we differ. I wish to hold open the possibility of a good outcome for others, regardless of my own experience and decision, and based on their own decision. You, by your own admission, have made that decision already, and wish others to make the same decision as you.
@Rob
How do you come to the conclusion that I wish others to make the same decision as I have? Particularly when I’ve just encouraged TW to take the vaccine if he wishes?
More OCD boxing.
Broadly speaking, I’m not particularly concerned how the vaccine plays out. My comments on it here are purely related to the extent to which it may or may not provide some timely relief to the airline industry. The article here says that the Pfizer vaccine is not going to be a silver bullet for the airline industry. I agree with that…no matter how much it annoys you to be confronted by an opinion that’s different to yours.
Bryce:
I think you are taking out of context and even mis quote.
The line is “It May Not Be A Silver Lining”
My take is why is Leeham even speculating on this? Its duplicitous and misleading that they don’t also acknowledge other vaccines in the works and they have their ramp up as well and its the whole picture that counts. So that is billions of doses total isn’t it?
It reeks of sour grapes. Yea and it might be a silver lining. Anyone with two brain cells can see we are not flipping a light switch here.
You don’t have to get a magnify glass out to see that the doses available are not huge by December end.
Well yea, they got to ramp up.
Rawlins does a deep dive and comes up with 4 years.
Man, what a prophet. Man I want him to run my investments!
And its not a select group that suffers Covd. I know of a number of athletes in top shape that it was hell for.
Your odds are worse as you get older, but the impact and symptoms are not age specific either.
220,000+ deaths (US only) are not something to sneeze at.
That includes young people that dies and we don’t know how compromise people heath is as they age do we?
You could suffer a stroke a heartbeat from now.
So, yes I fully respect any decision you make, but I don’t respect your experience is anything more than a very miner sub set of the data and possible consequences for people as a group.
Or to put it succinctly , your specif data sucks as a data set.
If you were a polio victim in an iron lung it would be different. You don’t know who is going to get the iron lung short straw (or crippled or dead) .
TW, go back and read the July post linked in the article.
Scott: I did fail to read the link which is more informative.
But its also disengerous and misleading that its just (Pfizer and BioNTech more accureaely) that is on the path and the sole answer.
There in fact are at least 6-8 vaccines in progress (discounting the Russian and Chinese)
And in fact the Pfizer and BioNTech vaccine is not viable in the less developed countries due to the Dry Ice ala very low temp requirement (-80c).
But Rawlins cites the quantity and cutting the number inoculated in half, yes we can do the math. Even I can manage that in my advanced dotterage.
Equally it may be a bust. But if you are going to use data to bust the bubble then your data should be in context and I don’t find it anything more than a grandstanding opening line (and then goes on to discuss tech details in the industry).
Meteor Is Going to Kill Us All! : Yea, maybe, but whats the relevance, whats the context.
Or even if its an outright failure we learn something.
Am I counting the chickens here? No. Do I find it intersing , yes.
And you might want to see Dr. Fauchi interview because his take is the same as mine.
Its hopeful, we need to see the data, then I will make a determination for myself and what I recommend to my wife.
Now that is spot on.
Bryce, this is baloney. You have gone after the value of the vaccine and derided both it and the efforts to produce it. Not just here or in this context, but in many other articles as well. I have defended it and will continue to do so.
I also agree the vaccine will not have any impact on the airline industry in the short term. But over time, it offers the potential for significant improvement, therefore should not be dismissed.
More OCD boxing.
You have difficulty distinguishing between verbs such as “observe”, “explain”, “defend” and “advocate”.
I’m not “deriding” any CoViD vaccine. Expressing strong doubts as to potential usefulness is not “derision”. There are plenty of virologists who express similar doubts: in fact, a whole swarm of them jumped on Monday’s news and warned that there were still many, many unanswered questions regarding vaccines. That’s called scientific discussion.
What I’m “deriding” is the idea that a vaccine will be a silver bullet that delivers us from all evil, and that we don’t have to try to develop any “plan B”. And I’m certainly “deriding” the fact that the aviation industry, in particular, is passively flushing itself down the toilet while it waits for this silver bullet.
I know that you’d love all noses to be pointed in the same direction on this subject, but that’s a delusion. Both on this forum, and in the world at large.
Bryce, there is a difference between your comments and those of the authors you quote.
Plenty of people have questions about the vaccine, myself included, that aren’t expressed in the negative context you invariably use. But I guess we just have to go on correcting for the negativity.
I don’t point the noses of the world. Governments are spending billions in this effort, which thus far has provided positive results. That’s not a coincidence, nor is it a delusion.
I completely agree with Scott, don’t get over-optimistic about a vaccine.
The major issue is going to be uptake as you point out. Even in the UK, you’d be surprised at the takeup / lack of takeup of the annual Flu vaccine.
I don’t remember the figures but even a known, stable Flu vaccine with well understood, and very mild side effects isn’t embraced by the population at the level a COVID vaccine would need to be to provide a solution to this issue.
In the UK, we have parents who still rely on others to vaccinate their children against Measles so that they can ‘believe’ that by refusing to vaccinate their own children, they are doing the best to protect their children from what they fear is vaccine (MMR) induced Autism. (It appears that the UK stripped Dr Andrew Wakefield of his medical licence in 2010), unfortunately, it seems that the damage is done, and social media allows this completely false perception to persist.
Add into this mix quite a number of people who are spreading the totally baseless claim that COVID is caused by 5G cell towers (even apparently in countries with absolutely no 5G towers at all). People spreading stories about this all being a hoax, and just governments wanting to implant chips into everyone to be able to control the population.
Most of the population doesn’t know anyone personally who has been admitted to hospital with, or died of COVID, and as such, they are less likely to understand just how real the pandemic is. They are fertile ground for conspiracy theories. The rules are treated as guidance, and to be followed by others.
As we’ve seen by the resurgence of Measles, the problem comes when too many people are leaving it to others to follow the rules.
We are failing as a society to educate people to understand, and use scientific method to determine the validity of what they assimilate through the media, especially through social media.
We don’t seem to be teaching people how to think critically, and to evaluate the data we consume.
(Of course politicians all over the world have decided to trash their economies, and make themselves hugely unpopular with their electorate at exactly the same time. They’ve decided to make millions of people unemployed with all the problems associated with that. ICU nurses have decided to do 6 days work every shift, and not have toilet breaks as it takes time to doff, and don your very uncomfortable PPE safely, utterly exhaust themselves, and suffer PTSD from what they are seeing… OR maybe, just maybe COVID-19 is real ?)
There is some evidence that if you’ve had COVID-19, and recover, immunity in some individuals anyway may only last 6 months, so it’s likely that the “herd immunity” thing isn’t going to solve the problem either. (2 positive tests in an individual 6 months apart after recovering from the 1st infection, and 2 completely different sequences i.e. not residual particles from the 1st infection).
So vaccines will help reduce mortality, and pre-infection, and recovery will slow transmission, but will a vaccine be the silver bullet ? No sadly not.
Things will improve, with time we’ll get better at treating COVID with new therapeutics, more vaccines will complete trials, and be introduced into the fight against COVID, but it’s not going to happen by Christmas.
Indeed.
A key sentence in the link that I posted above is:
“Another challenge with the vaccine is that young people, who don’t tend to get as sick as people over 40, may not think they are at high risk for severe health outcomes if they get the virus. If they hear about side effects via word of mouth, they may not deem the vaccine to be worth it.”
Agreed.
From an article at the end of 2018…
“Only 25% of social care staff looking after the elderly and vulnerable are vaccinated against flu, report says”
https://www.theguardian.com/society/2018/oct/18/mps-shocked-by-low-flu-vaccine-rates-among-social-care-staff
It also states: “Health workers have been told they have a professional duty to be vaccinated, and the takeup rate across the NHS was the highest ever, at 68%. But that hid huge variation across England, says the committee. Some trusts only managed 30–40% while others achieved 90%.”
I know it has improved over the last few years, but even if it was 80% across the NHS (UK National Health Service), it’s nothing like that across the general public.
The percentage of the population you’ll need to vaccinate against COVID-19 depends on a few things, amongst others; the efficacy of the vaccine, and the proportion of the population already infected, recovered, and immune to further infection.
If you were to vaccinate 100% of the population you’d need a vaccine with 60% efficacy. At 75% of the population, your efficacy has to be around 70%. At 60% of the population covered, you need 80% efficacy. So good news if the Pfizer vaccine has 90% efficacy, but we’d still have to get near to half the population to accept vaccination.
Perhaps a requirement for inter country travel should be mandatory vaccination ? 50 years ago people travelling from countries in Africa to the UK had to produce documentation that they’d been vaccinated against various diseases.
@ JakDak
“Perhaps a requirement for inter country travel should be mandatory vaccination ?”
I think that quite a few countries — and perhaps a few airlines — may take such an approach…although you then have the headache of trying to come up with an acceptable, fraud-proof, international vaccination certification system…something that nobody appears to be working on at present. Even better: augment such a certification system to include antibody and/or T-cell titer, so that recent post-CoViD patients are also covered to travel for a limited period. In fact, that latter aspect could be implemented at present, if any relevant authority had the will and saw the potential.
Even today, if you try to enter several Asian countries following a stay in certain African countries, then you must present evidence of a yellow fever vaccination.
In the US, receptivity to the initial vaccine is about 40%. Another 25% would accept the vaccine if proven safe in the trials and initial rollout. So 50% is very achievable, again with truthful messaging.
Prior to Trump’s political attacks on Fauci and Birx, in an attempt to win the election, the US initial percentage was around 70%. So significant damage was done by the negative messaging, but it can be reversed over time with truthful messaging.
BC had a problem with the irresponsible nurse’s union and a one-employer system.
Otherwise the employer could just stay vaccination is the rule, id you don’t like that move on.
(That’s to counter TW’s snide Marxist remark “(if a businessman says it it must be true)” :-o)
JakDak, I don’t think anyone (besides possibly Trump) has claimed the pandemic will be over by Christmas.
The point is that if the Pfizer trials really do have an efficacy of 90%, that bodes well for the other vaccines that are now in trials. If they come out to be similarly high, each of those likewise has millions of dosages already on hand, with manufacturing ramping up. So within two years, we could have enough vaccine for the majority of the population.
The 6 month claim for immunity is based on how far we are into the pandemic and the research that has been done thus far, mostly on the primary response antibodies (first-responders). There is also research to suggest that immunity from other mechanisms lasts longer, and that the vaccine does provoke those same responses. The manufacturers are saying they are expecting a year, but we don’t yet know how long it will last. It could be years before we know for sure. But that’s not a reason to denounce the vaccine.
We can look at the pandemic data to get an idea of this. Thus far there is no evidence of large numbers of people who were infected being re-infected. So that implies the immunity lingers, and that should also be reflected in the vaccine results.
As far as uptake rate, the messaging matters enormously. Yes, there will always be the 5G crowd, anti-vaxxers, flat-earthers, 9/11 conspiracists, Apollo conspiracists, and others. And we will now add several new categories for COVID conspiracies. The common thread for all of them is to deny the scientific evidence and be skeptical of anything that goes against their personal convictions. They have already decided for themselves, and now wish to promulgate their views to others.
But these remain a small portion of the population, and the rest are still accessible by messaging. So there will be a battle in cyberspace for those minds, positive vs negative messaging. Many of the deniers will attempt to preclude acceptance by sowing doubt and distrust before the data are even fully available.
And the more positive the data are, the louder those voices will become. They will attack the experts and the data. They will imply bias in the results to create bias in acceptance. They will engage in “outlier science”, finding a negative opinion and proclaiming it’s the “real” truth, in defiance of the consensus of the medical community. They will imply horror stories about reactions to the virus. They will insist people won’t accept it, in hopes that people won’t accept it. We have seen these methods employed already in these pages.
The reason the trials require anonymity for public discussion by members, is to protect them from attack by groups that seek to undermine the results. That is a truly shameful thing, but a reality nonetheless. If such a person posted here, they would be attacked and criticized, even while volunteering to help establish a scientific basis for the vaccine.
But we’ve also just seen an election where these same methods were attempted to disrupt the vote, yet ultimately rejected by the population, who voted by mail in unprecedented numbers. So it’s not an impossible goal.
We have the scientific truth, the experts, and the medical community, and these things can be used to great effectiveness, with truthful messaging. Most people support and trust Dr. Fauci in spite of the numerous attacks on him. There are others like him, and he hasn’t backed away from the challenge. He’s been truthful and straightforward and people will respond to that. And most importantly, that is true whether the vaccine results are positive or negative. If they are negative, Dr Fauci would report and advise on that with equal veracity. As would all the involved scientists.
So yes, there is a battle ahead, and much depends on the data that are still to come. But if the data remain positive, with the right message, it can be won despite the naysayers.
Anyone who posts responsibly, should think about the audience and potential impact of negativity at this early stage. You can praise the positive results while also asking questions to be answered, raising concerns or proposing solutions regarding future issues. This is how scientists factually respond to the work of other scientists. We can set that example, if we choose.
Re the following in Bryce’s post above: ” However, upon closer inspection, the magnitude of these effects is not to be taken lightly: one subject woke up in the middle of the night (after his second dose) with shivers that were severe enough to cause him to break a tooth, and fevers of 104 F / 40 C were not uncommon.”
The following is provided for anyone who is interested how the side effects actually reported by Pfizer/Biontech for all 72 patients in the phase 1/2 study of their phase 3 COVID-19 vaccine candidate, compare to those reported by CNBC based on interviews of 5 patients – “three in Moderna’s study and two in Pfizer’s late-stage trials”.
“Systemic events in response to BNT162b2 were milder than those to BNT162b1 (Figures 3, S1, and S2). For example, only 17% of 18–55 year olds and 8% of 65–85 year olds reported fever (≥38.0–38.9°C) after Dose 2 of 30 µg BNT162b2. Severe systemic events (fatigue, headache, chills, muscle pain, and joint pain) were reported in small numbers of younger BNT162b2
recipients, but no severe systemic events were reported by older BNT162b2 recipients. There were no reports of Grade 4 systemic events by any BNT162 recipient. Overall, systemic events reported by 65–85 year olds who received BNT162b2 were similar to those reported by those who received placebo after Dose 1. ”
https://www.medrxiv.org/content/10.1101/2020.08.17.20176651v2.full.pdf
I am enrolled in phase 3 of the Pfizer COVID vaccine study (approximately 44,000 participants) and have had no side effects at all. While I do not know whether I am in the vaccine or placebo arm, my case manager has told me that far more than half of the participants are reporting no side effects. Since participants are split 50/50 between the placebo and vaccine arms, this means that many in the vaccine arm are reporting no side effects, consistent with the results from the phase 1/2 study that I quoted above.
Great that you’ve had no side effects.
When the results of the much larger-scale Phase 3 trials are included (nominally 44,000 participants) instead of just the phase 1/2 trial (72 participants) then one does start to get occurrences of severe / grade 4 side effects….albeit rare. This is to be expected, seeing as the statistical base size is greater, and the trial population is more diverse.
https://www.hospimedica.com/covid-19/articles/294784562/pfizers-covid-19-vaccine-shows-mild-to-moderate-side-effects-in-phase-3-clinical-trial.html
Re in Bryce’s Post Above: “I can very much imagine that GPs will be reticent about subjecting frail old ladies to the risk of a 104F fever and teeth-breaking shivers.”
No fever above 38.9 C = 102.0 F was reported by Pfizer for 18 to 55 year olds in the phase 1/2 study of their phase 3 COVID-19 vaccine candidate (BNT162b2 – see page 18 at the link below).
No fever above 38.4 C = 101.1 F was reported by Pfizer for 65 to 85 year olds in the phase 1/2 study of their phase 3 COVID-19 vaccine candidate (BNT162b2 – see page 20 at the link below).
https://www.medrxiv.org/content/10.1101/2020.08.17.20176651v2.full.pdf
My case manager in the Pfizer phase 3 COVID-19 vaccine study that I am enrolled in, told me that at that particular clinical site, the highest temperature that they had seen in an older adult was about 100 F.
Thanks so much for this, the truth is really important to put out there, positive or negative. Everything I have found on this indicates the reactions have been similar to the flu vaccine.
Thank AP. You are the guy with data for sure.
Bryce:
I do get your view, but no different than mine on vaccines when I was a kid (not that I had a choice).
Neither one of us is a good data set. It takes 10s of thousands.
So lets see how it plays out?
Frankly I am no match whiz (ok but get into deep data dives, ungh).
I can read the synopsis and make as best a decision as possible.
I do that each day driving (well assuming I drive that day).
So far I am up to the task! I am hopeful the next time I go driving I am again.
That is a data set of 100s of thousands of miles of driving. So I have a pretty good data set.
Sadly I am getting older (me and Scott!) Call it fortune or unfortunate I have had to test my skills in lock to lock reaction (ice sucks and a rig with a bad balance on ice sucks even worse). Yep, I did it, as good short term as when I was 25.
Ok, I am pretty confident I still have it.
I am not confident or confidant on the vaccine, I am hopeful and will see what the data tells us in the next couple of months.
104 is dangerously high. Into an ice bath!
A daughter had 105 once circa age 9, because clever medical people had lowered age for vaccination against measles to protect younger, but there was a significant incidence rate of it not being effective. Practice changed to add a second several years after the first.
I had 105 once from reaction to a strong sulfa antibiotic or such medicine cocktail.
Measles, Mumps Rubella vaccines are given (free of charge) in New Zealand at 2 and 3 years of age. None of my 4 children, nor my 11 grandchildren, have had the slightest reaction. The real data shows vaccination to be VERY safe. And, of course, those vaccinated do not get those diseases.
Yes, while side effects and negative reactions are possible with individuals for any vaccine, the incidence rate is low and in general they are very safe.
The anti-vaxxers have worked hard to defeat that message, but it remains true nonetheless.
Vaccination is routine in the US and required for public school enrollment. Parents can file a form to object, with a doctor’s note recommending the child not be vaccinated. Some states also have religious grounds for objection. The school retains the right to deny admission if that illness occurs in the school, or in the child, for liability reasons.
On the subject of the MAX :
Lessors are (logically) indicating that the EU tariffs on Boeing products could impede MAX uptake in the EU:
https://www.reuters.com/article/us-air-lease-tariffs/european-tariffs-on-boeing-planes-threaten-their-deployment-in-europe-lessor-idUSKBN27Q00M
Biden will probably (try to) put an end to this endless fueding, but that’s still months away.
Well not that many deliveries right now so we can wait.
On the to do list Covd tops it all.
And Pfizer vaccine needs to be kept at -80°C, so not easy to distribute!
Yes, the length of time that refrigeration can be substituted for freezing is being investigated. The vaccine is shipped in dry ice which can last for about a day with adequate packaging.
The major air shippers such as UPS and FedEx have been aware of this and have been setting up freezer locations around the world, and experimenting with packaging. That has been part of the vaccine development effort, and is funded by the US government.
@tooper
Update on logistics of cold distribution
https://www.bbc.com/news/technology-54889084
https://www.bloomberg.com/news/articles/2020-11-10/deep-freeze-challenge-makes-pfizer-s-shot-a-vaccine-for-the-rich
https://www.propublica.org/article/most-states-arent-ready-to-distribute-the-leading-covid-19-vaccine
Two things struck me: one is insulated boxes are only currently available certified for storage down to -8C (so not suitable for low temperature medicines which need around -18C, but probably a good option for medium temperature cold storage). The Bloomberg (and the WSJ article which lead coverage) referred to Pfizer’s solution being capable of maintaining -70C (so they’ve already been bartering themselves down from previous statements saying the vaccine needed -80C — I’m always on alert when what should be absolute technical details start getting fuzzied). They mention dry ice as a source of thermal absorption, which without built-in mechanical cooling on the storage box can’t reach down to -80C. Nor do Pfizer mention any testing or product certification having been carried out. The timeframe for maintaining box temperate was also vague — it will have to have, by the laws of thermodynamics, different performance curves in high ambient air temperature regions for instance and it wasn’t spelt out if the quoted temperature maintainability time was relying on being in placed either a medium or low temperature refrigerated environment.
The other thing Pfizer ‘fessed up to was the phials were only capable of withstanding 4 exposures to ambient air without compromising stability. A logical guess is that embrittlement of the pharmaceutical-grade seals on the phials caused by any repeated thermal stress eventually means there’s soo much risk of allowing any more. So, four strikes and you’re out. You can envisage one exposure to ambient air as the vaccine leaves the the vaccine finishing plant and gets packed for initial transportation to the bulk storage facility. Another exposure will occur when they’re unpacked and placed into bulk storage. Then another exposure when they’re lifted out of bulk storage and repacked for local distribution. There’s one “life” left after all that — unpacking and thawing prior to dispensing. So zero room for any errors or unintended ambient air exposure.
For a Big Pharma player who must know there’s going to be a lot of scrutiny about quality control and vaccine safety, I don’t get why they think vague musings to tame press outlets and “tah-dah!” hero techie fixes like the storage box are going to cut it.
@ Gerrard White
A neat summary.
Of course certain people won’t like it, because it’s far too realistic and confronting for them.
Here’s another pickle: if an unintended mishap occurs somewhere during transport of a batch, e.g. an unintended temperature breach, will it come to light…or will it be covered up, and a dud batch administered to unsuspecting recipients? I once had a client who had to transport ultra-sophisticated apparatus at a highly controlled temperature: after multiple incidences of shoddy transport, he eventually resorted to putting temperature sensors in his shipments to record the temperature during the entire transport trajectory.
Another interesting question: what’s the projected cost per dose of the elaborate transport procedures required? The cost of the vaccine itself for the entire world population is half a trillion dollars ($35 per shot)…excluding transport.
The solution for any vaccine delivery network is managing the time-temperature-life dependence.
Pfizer has reported that specialized cold storage freezers at the ideal temperature of -80 C can support a vaccine life of 6 months. Their cold storage shipping containers can sustain the vaccine for 10 days, extending to 15 days with refill of dry ice. Transfer to ordinary freezers provides a life of up to 5 days. Transfer to ordinary refrigerators provides a life of up to 1 day. Exposure to ambient requires immediate use or disposal.
So this is a manageable problem. There is sufficient margin to accomplish distribution and application. Pfizer is using their own supply chain, including real-time electronic telemetry and tracking, to ensure vaccine quality and calculate remaining life within the chain.
For other vaccines such as Moderna, McKesson will manage the supply chain, and already have the capacity to distribute about 200 million doses, with adequate refrigeration capacity. Ordinary freezers at -20 C are sufficient for long-term storage and transport. Ordinary refrigerators provide a life of 7 days.
I’ve written freezer management software in use at universities with large genetics research departments. They have the same problem in terms of optimizing freezer inventories, orders, and usage, to avoid expiration and spoilage of extremely expensive products (a typical freezer might contain $50K to $100K).
Another issue was providing backup solutions for power failure. We measured and tracked freezer temperature rise and staff were assigned as first responders, with a large cache of dry ice on-hand. It’s really nothing new for people experienced in this area, been going on for a long time.
As time went on, the manufacturers began to provide both freezers and management, the advantage being they would absorb any expiration or spoilage as long as the bulk shipping packs were not opened. They used remote telemetry as well. So they too are experienced in this area.
@Bryce
Another skeptical comment from the Ultra Establishment Foreign Policy site
It seems that Pfizer, when they talk about distribution have restricted their PR to the US, and appear to mean ‘distribute to relevant state authorities’
While no manufacturer appears to have a thought through distribution plan, it might be apparent that they expect ‘the authorities’ to pay
Costing one out? Not likely
https://www.statnews.com/2020/11/11/rural-hospitals-cant-afford-freezers-to-store-pfizer-covid19-vaccine/
Although reading a Plan in a Press Release is ungrateful work
FP, as others, have raised the all important reluctance of the US population to take a vaccine in the numbers required for any ‘overall’ success
Note that in the Pfizer distribution plan, there is no expectation or need for hospitals to have the specialized freezers. The plan assumes the standard hospital freezers will be used, and allows for that.
Acceptance is a work in progress. The US willingness was damaged by the disinformation campaign to cast doubt on the severity of COVID or need for precautions, which has spilled over into vaccine resistance. And that resistance also has its own disinformation campaign from the anti-vaxxers.
Ironically, the disinformation sources which provide the negative messaging, also point to the results as supportive of their cause. Classic case of self-fulfilling prophesy. You claim something is true, then work to cause it. Prior to the campaign, the US willingness was around 70%.
The CDC and NIH know they have a task ahead of them in terms of positive messaging and outreach. They’ve been preparing for that and have communications programs ready. But the vaccine needs to be understood and approved before they can be rolled out.
Once that happens, the anti-vaxxers won’t have the stage to themselves any longer. That will be a welcome relief.
Dry Ice will keep it that cold and colder, they have been doing it for a long time. Its not new.
Also it can be refrigerated for a week and ok.
It can be thawed for a couple of hours and ok.
It can be and will be managed with GPS and temp monitoring system.
Its not good news for the developing world but if the Developed countries can get back to normal we can get the vaccines that just need to be cool out to them.
They can’t develop any of this and we can. Life is not fair, and I am truly sorry for them but we can also ensure they are not left dangling.
Regarding in Bryce’s post above: “Here’s another pickle: if an unintended mishap occurs somewhere during transport of a batch, e.g. an unintended temperature breach, will it come to light…”
Pfizer’s has equipped it’s shipping containers with GPS trackers with temperature sensors that report location and temperature data in real time to verify that correct temperature was maintained during shipment. If the GPS tracker and temperature sensor reports that an unacceptable temperature deviation occurs in a container, the vaccine in that container will not be used. See the following excerpt from the article at the Pharmaceutical Commerce at the link after the excerpt.
“He notes that uncertainty about the cold-chain capabilities of transportation providers and vaccine administration facilities resulted in Pfizer developing a special cooler, or “thermal shipper,” with real-time GPS and thermal monitoring that can maintain deep-freeze vaccine storage for 10 days if left unopened.”
https://www.pharmaceuticalcommerce.com/latest-news/pfizer-to-coordinate-its-own-coronavirus-vaccine-distribution/
From CNN:
https://www.cnn.com/2020/11/10/health/pfizer-vaccine-distribution-cold-chain/index.html
‘ State health officials were “shocked” when they heard the storage requirements for the new vaccine, according to Dr. Kelly Moore, associate director of the Immunization Action Coalition, which is supporting the frontline workers who will administer the coronavirus vaccine. Those requirements include procuring and handling large amounts of dry ice, which is in short supply in many parts of the country.
“We all are going into this expecting that there are going to be major glitches,” she said.
Howell, North Dakota’s immunization program manager, calls the prospect of administering Pfizer’s vaccine “overwhelming” and “daunting.”
Claire Hannan, executive director of the Association of Immunization Managers, which also helps states with their vaccine programs, sent Howell the exploding head emoji.
“These challenges are so unprecedented. I don’t have anything to compare [them] to,” Hannan told CNN.
Even those on the inside have doubts about how the process is going.’
‘ In the past, the CDC has managed relationships with state health agencies, but during the pandemic, the CDC has been sidelined, and is now doing the work along with Operation Warp Speed.
That has not always gone smoothly, with “an element of having too many bosses,” said Laurel Wood, coordinator for public health for the Immunization Action Coalition. “There are many cooks involved.”
While the CDC historically has enjoyed good relationships with state health departments, she said there’s been some tension between Operation Warp Speed and the states.
One state program manager was “almost in tears” after receiving a “castigation” by an Operation Warp Speed official who was unhappy with a plan she filed, Wood said.
“You’ve got people coming at you from a thousand different directions.” ‘
‘ At Pfizer’s webinar with state health officials last month, the company laid out its specific requirements.
Once sites receive their thermal shippers filled with vaccine, they’re supposed to replenish the dry ice within 24 hours. If they don’t use the vaccine within five days, they’re supposed to replenish the dry ice again, and then again five days later.
Clinic staff must act fast when removing vaccine from the shippers. According to Pfizer’s instructions, the boxes can be opened only twice a day, and each time for no more than a minute.
At any point, the vaccine can be removed from the shipper and put in the refrigerator, where it is good for only five days — any longer than that and the vaccines have to be thrown away. When ready to use, nurses dilute the vaccine, making five doses with one vial. Those five shots have to be given within six hours. If more than six hours pass, the vaccines have to be thrown out.
This whole process has to happen twice for each patient, since the vaccine is given in two doses spaced three weeks apart.
That’s why heads began to explode on the Pfizer webinar, according to five people who attended it.
Health care workers have never had to procure dry ice before, much less when it’s in short supply, as it is in some parts of the country. Handling dry ice can be hazardous — it can burn the skin, and in spaces with poor ventilation, can produce potentially deadly fumes.
There’s another potential problem. Doctors and nurses overtaxed with Covid-19 patients and other responsibilities will be challenged to follow directions perfectly — directions where mere minutes matter.
“They’re all so insanely busy,” said Moore, the doctor who’s helping doctors and nurses get ready.
“I know they were astonished when they got their first glimpse from Pfizer on all of the steps in this process, on the thermal shipper and how it worked,” she said. “You could see all of the brains spinning.” ‘
@Pedro
Gerrard White posted that same link the other day…though it’s always good to re-post relevant information.
But most people just don’t know what it entails to produce and maintain temperatures like this, so they’re puzzled as to why this could possibly be posing a challenge. After all, the mail gets delivered every day, doesn’t it?
What I found especially interesting in this article is that CNN asked Pfizer if the “magic boxes” had been tested…but there was no reply. I’d *really* love to know what type of magical thermal insulation is present in those boxes to be able to keep dry ice from sublimating without any assistant refrigeration mechanism…*for days*. I wonder if the Pfizer people have ever left ice cubes in a cooler for a few hours to see what happens?
I read yesterday that the distribution is so challenging that Pfizer will be doing it itself rather than using the recommended courier company. However, they’ll still just be dumping it off at relatively coarse “state level”, leaving it up to local authorities to solve the finer-scale distribution.
I have a nasty suspicion that, if the Moderna vaccine (normal refrigeration) is available within a similar time frame, then it will quickly win over from this ultra-cold nightmare. A possible exception will be in big cities.
A lot of misunderstanding here. The task that’s being “dumped” on the state level is administering the vaccine to patients. When they say where and when the vaccine is needed, that will be where and when the vaccine will be delivered.
So endpoints will be responsible for maintaining their inventory within the constraints of the cold chain. If they ever have more than a few days of supply on hand, something is wrong. One shipping container (about the size of a suitcase) contains 1,000 to 5,000 doses. So it’s not some huge storage requirement.
While outpatient clinics are not accustomed to this kind of storage, hospitals are, as I mentioned the cold chain has been in place for a very long time for researchers. So the expertise exists, but it will be required at a new level now.
I’m sure there will be a learning curve for the end care workers, but they will have support. Handling dry ice is not that difficult, the ice cream industry has done it for many years.
As far as the shipping containers, there is no magic involved, it’s a simple heat transfer problem. The dry ice is contained in vented pouches so can be handled with gloves. Swapping the pouches is all that’s needed. The rate of replacement is known and the temperature of the vaccine is monitored to ensure enough refrigeration is present.
Since dry ice sublimates rather than melting like water ice, the heat absorption is about twice that of water ice. The thermal mass of the vials is small relative to that of the dry ice.
So the determining factor is the insulation of the container. In the videos I’ve seen, there is several inches of specialized foam insulation, probably 10 times that of an igloo cooler.
It’s a challenge for sure, but not insurmountable. Mostly a matter of education and learning to manage it well.
One caution is that dry ice can be hazardous to shippers, they have to keep in top of mind that too much CO2 in confined spaces can kill. (‘dry ice’ being frozen CO2)
No, it’s not the climate alarm scam Bjorn falls for, besides displacement of oxygen there is a threshold of lung function impairment.
So don’t stuff the package in the back of the flight deck, as I was told was the practice for medical isotopes. Don’t fill your small delivery van full of packages with dry ice unless you can organize good ventilation.
(On site in Cranbrook BC looking through the pieces of PW 314, we were alerted to the shipment of a package of radioactive medical isotopes, but records did not specify whether it had been placed in a cargo compartment with airline paperwork or in the flight deck for security and quick access. But then we were advised that it was moot as the half-life was very short, that’s why it was sent by air.
Such isotopes usually came out of a nuclear facility in ON. After the fiasco of that facility being taken offline for essential unplanned maintenance that should have been prevented, scientists developed a way to make many of the isotope types in small cyclotrons such as the university in Edmonton AB and other locations around the world had. The pilot facility was built in the big TRIUMF cyclotron facility in Vancouver BC by various researchers including some retired ones. IIRC UA is one of the Tri universities in TRIUMF, which eased transfer of technology to its example of a small facility.)
I understand that temperature logging has long been available, quite small devices now, could even be read with RFID at intermediate points I expect.
Packages need to be tamper-resistant.
There is risk of stupid/dishonest delivery people IMO.
Amazon and other couriers are not top quality. I just had a circus of a new contractor company for Amazon repeatedly trying to deliver a package to a commercial facility after hours. Indications are the actual delivery person was keen but dense. And earlier I had a transportation operation send me an excited email saying my high-value attractive-to-steal package was almost to my location – coming out of Florida it had cleared the Border Barrier into Ontario, so maybe was halfway. Don’t they teach geography in school? (Answer NO – a huge proportion of HS students in Minneapolis and Winterpeg did not have a clue where the other city was. Never mind the big river between them.)
Regarding cold storage issues with the Pfizer-Biontech vaccine – They have so far done well enough at the following network of 154 phase 3 study sites in the USA, Argentina, Brazil, Germany, South Africa, and Turkey, with whatever cold storage requirements there may be, to demonstrate effectiveness of over 90% in the vaccine arm of the study in the analysis of the first 94 participants in the 44,000 patient study who developed COVID-19 symptoms. Half of the participants got vaccine and half got placebo. In big USA cities some of the study sites are large University Hospitals that may have special refrigeration equipment; however, many of the study sites in small and medium USA cities are community clinical research operations that are operated by family practice clinics that have no special refrigeration equipment. The clinic in Idaho where I am enrolled in the study is one such clinic. They schedule a certain number of patients per day for vaccination, and then order the appropriate number of vaccine doses from the special refrigeration facilities for that day’s or a few day’s patients. Kind of like going to the store and buying enough perishable food for the next few days, but not so much that the food will go bad before you can use it.
United States, Alabama
North Alabama Research Center, LLC
Athens, Alabama, United States, 35611
Birmingham Clinical Research Unit
Birmingham, Alabama, United States, 35216
Medical Affiliated Research Center
Huntsville, Alabama, United States, 35801
Optimal Research, LLC
Huntsville, Alabama, United States, 35802
Alliance for Multispecialty Research, LLC
Mobile, Alabama, United States, 36608
United States, Arizona
Chinle Comprehensive Health Care Facility
Chinle, Arizona, United States, 86503
Johns Hopkins Center for American Indian Health
Chinle, Arizona, United States, 86503
The Pain Center of Arizona
Phoenix, Arizona, United States, 85018
HOPE Research Institute Recruiting
Phoenix, Arizona, United States, 85023
Alliance for Multispecialty Research, LLC
Tempe, Arizona, United States, 85283
Whiteriver Indian Hospital
Whiteriver, Arizona, United States, 85941
United States, California
Anaheim Clinical Trials, LLC
Anaheim, California, United States, 92801
Collaborative Neuroscience Research, LLC
Long Beach, California, United States, 90806
Long Beach Clinical Trials Services Inc.
Long Beach, California, United States, 90806
Kaiser Permanente Los Angeles Medical Center
Los Angeles, California, United States, 90027
National Research Institute
Los Angeles, California, United States, 90057
Providence Clinical Research
North Hollywood, California, United States, 91606
Paradigm Clinical Research Center
Redding, California, United States, 96001
UC Davis Medical Center
Sacramento, California, United States, 95817
California Research Foundation
San Diego, California, United States, 92123-1881
Kaiser Permanente Santa Clara
Santa Clara, California, United States, 95051
Bayview Research Group
Valley Village, California, United States, 91607
Diablo Clinical Research, Inc.
Walnut Creek, California, United States, 94598
United States, Colorado
Lynn Institute of Denver
Aurora, Colorado, United States, 80012
United States, Connecticut
Clinical Research Consulting, LLC
Milford, Connecticut, United States, 06460
Yale Center for Clinical Investigations (CSRU)
New Haven, Connecticut, United States, 06519
United States, Florida
Alliance for Multispecialty Research, LLC-Coral Gable
Coral Gables, Florida, United States, 33134
DeLand Clinical Research Unit
DeLand, Florida, United States, 32720
Fleming Island Center for Clinical Research
Fleming Island, Florida, United States, 32003
Indago Research & Health Center, Inc.
Hialeah, Florida, United States, 33012
Research Centers of America
Hollywood, Florida, United States, 33024
Jacksonville Center for Clinical Research
Jacksonville, Florida, United States, 32216
Clinical Neuroscience Solutions, Inc.
Jacksonville, Florida, United States, 32256
Acevedo Clinical Research Associates
Miami, Florida, United States, 33142
Clinical Neuroscience Solutions, Inc.
Orlando, Florida, United States, 32801
United States, Georgia
Atlanta Center for Medical Research
Atlanta, Georgia, United States, 30331
IACT Health
Columbus, Georgia, United States, 31904
Meridian Clinical Research, LLC
Savannah, Georgia, United States, 31406
Clinical Research Atlanta
Stockbridge, Georgia, United States, 30281
United States, Hawaii
East-West Medical Research Institute
Honolulu, Hawaii, United States, 96814
United States, Idaho
Solaris Clinical Research Recruiting
Meridian, Idaho, United States, 83646
United States, Illinois
Optimal Research, LLC
Peoria, Illinois, United States, 61614
United States, Iowa
University of Iowa Hospitals & Clinics
Iowa City, Iowa, United States, 52242
United States, Kansas
Alliance for Multispecialty Research, LLC
Newton, Kansas, United States, 67114
Alliance for Multispecialty Research, LLC
Wichita, Kansas, United States, 67207
United States, Kentucky
Kentucky Pediatric/ Adult Research
Bardstown, Kentucky, United States, 40004
United States, Louisiana
Benchmark Research
Metairie, Louisiana, United States, 70006
Ochsner Clinic Foundation
New Orleans, Louisiana, United States, 70121
LSUHSC-Shreveport Clinical Trials Office
Shreveport, Louisiana, United States, 71101
LSUHSC-Shreveport
Shreveport, Louisiana, United States, 71103
United States, Maryland
Pharmaron CPC, Inc.
Baltimore, Maryland, United States, 21201
University of Maryland, Center for Vaccine Development and Global Health
Baltimore, Maryland, United States, 21201
Center for Immunization Research Inpatient Unit
Baltimore, Maryland, United States, 21224
United States, Massachusetts
Boston Medical Center
Boston, Massachusetts, United States, 02118
UMass Memorial Medical Center – University Campus
Worcester, Massachusetts, United States, 01655
United States, Michigan
Michigan Center for Medical Research
Farmington Hills, Michigan, United States, 48334
United States, Mississippi
MedPharmics, LLC
Gulfport, Mississippi, United States, 39503
United States, Missouri
Clinical Research Professional
Chesterfield, Missouri, United States, 63005
Sundance Clinical Research, LLC
Saint Louis, Missouri, United States, 63141
United States, Montana
Bozeman Health Deaconess Hospital dba Bozeman Health Clinical Research
Bozeman, Montana, United States, 59715
United States, Nebraska
Methodist Physicians Clinic / CCT Research
Fremont, Nebraska, United States, 68025
Meridian Clinical Research, LLC
Norfolk, Nebraska, United States, 68701
Quality Clinical Research, Inc.
Omaha, Nebraska, United States, 68114
Meridian Clinical Research
Omaha, Nebraska, United States, 68134
United States, Nevada
Wake Research-Clinical Research Center of Nevada, LLC
Las Vegas, Nevada, United States, 89104
United States, New Jersey
Amici Clinical Research
Raritan, New Jersey, United States, 08869
South Jersey Infectious Disease
Somers Point, New Jersey, United States, 08244
United States, New Mexico
Johns Hopkins Center for American Indian Health
Gallup, New Mexico, United States, 87301
Johns Hopkins Center for American Indian Health
Shiprock, New Mexico, United States, 87420
United States, New York
Meridian Clinical Research, LLC
Binghamton, New York, United States, 13901
Meridian Clinical Research LLC
Endwell, New York, United States, 13760
NYU Langone Health
New York, New York, United States, 10016
Icahn School of Medicine at Mount Sinai
New York, New York, United States, 10029
Rochester Clinical Research, Inc.
Rochester, New York, United States, 14609
Rochester Regional Health/Rochester General Hospital
Rochester, New York, United States, 14621
SUNY Upstate Medical University
Syracuse, New York, United States, 13210
United States, North Carolina
PMG Research of Raleigh, LLC d/b/a PMG Research of Cary
Cary, North Carolina, United States, 27518
PMG Research of Charlotte LLC
Charlotte, North Carolina, United States, 28209
Duke University Medicine Circle- Duke Early Phase Clinical Research Unit
Durham, North Carolina, United States, 27710
PharmQuest
Greensboro, North Carolina, United States, 27408
PMG Research of Hickory, LLC
Hickory, North Carolina, United States, 28601
PMG Research of Raleigh, LLC
Raleigh, North Carolina, United States, 27609
M3 Wake Research, Inc.
Raleigh, North Carolina, United States, 27612
PMG Research of Salisbury, LLC
Salisbury, North Carolina, United States, 28144
PMG Research of Wilmington, LLC
Wilmington, North Carolina, United States, 28401
PMG Research of Winston-Salem, LLC
Winston-Salem, North Carolina, United States, 27103
United States, North Dakota
Lillestol Research LLC
Fargo, North Dakota, United States, 58104
United States, Ohio
Sterling Research Group, Ltd.
Cincinnati, Ohio, United States, 45219
Cincinnati Children’s Hospital Medical Center
Cincinnati, Ohio, United States, 45229-3039
Sterling Research Group, Ltd.
Cincinnati, Ohio, United States, 45246
University Hospitals Cleveland Medical Center
Cleveland, Ohio, United States, 44106
VA Northeast Ohio Healthcare System
Cleveland, Ohio, United States, 44106
Rapid Medical Research, Inc.
Cleveland, Ohio, United States, 44122
Aventiv Research Inc.
Columbus, Ohio, United States, 43213
Dayton Clinical Research
Dayton, Ohio, United States, 45406
PriMED Clinical Research
Dayton, Ohio, United States, 45419
Senders Pediatrics
South Euclid, Ohio, United States, 44121
United States, Oklahoma
Lynn Institute of Norman
Norman, Oklahoma, United States, 73069
United States, Oregon
Kaiser Permanente Northwest-Center for Health Research
Portland, Oregon, United States, 97227
United States, Pennsylvania
Lehigh Valley Health Network/Network Office of Research and Innovation
Allentown, Pennsylvania, United States, 18102
United States, Rhode Island
Omega Medical Research
Warwick, Rhode Island, United States, 02886
United States, South Carolina
Main Street Physician’s Care
Little River, South Carolina, United States, 29566
Main Street Physician’s Care
Loris, South Carolina, United States, 29569
United States, South Dakota
Meridian Clinical Research
Dakota Dunes, South Dakota, United States, 57049
United States, Tennessee
Holston Medical Group
Bristol, Tennessee, United States, 37620
Holston Medical Group
Kingsport, Tennessee, United States, 37660
Alliance for Multispecialty Research, LLC
Knoxville, Tennessee, United States, 37920
Clinical Neuroscience Solutions, Inc.
Memphis, Tennessee, United States, 38119
Clinical Research Associates, Inc.
Nashville, Tennessee, United States, 37203
Trinity Clinical Research
Tullahoma, Tennessee, United States, 37388
United States, Texas
Benchmark Research
Austin, Texas, United States, 78705
ARC Clinical Research at Wilson Parke
Austin, Texas, United States, 78726
Tekton Research, Inc.
Austin, Texas, United States, 78745
North Texas Infectious Diseases Consultants, P.A.
Dallas, Texas, United States, 75246
Ventavia Research Group, LLC
Fort Worth, Texas, United States, 76104
Benchmark Research Recruiting
Fort Worth, Texas, United States, 76135
University of Texas Medical Branch
Galveston, Texas, United States, 77555
Ventavia Research Group, LLC
Houston, Texas, United States, 77008
Texas Center for Drug Development, Inc.
Houston, Texas, United States, 77081
Ventavia Research Group, LLC
Keller, Texas, United States, 76248
SMS Clinical Research, LLC
Mesquite, Texas, United States, 75149
LinQ Research, LLC
Pearland, Texas, United States, 77584
Benchmark Research.
San Angelo, Texas, United States, 76904
Clinical Trials of Texas, Inc.
San Antonio, Texas, United States, 78229
Diagnostics Research Group
San Antonio, Texas, United States, 78229
Martin Diagnostic Clinic
Tomball, Texas, United States, 77375
United States, Utah
J. Lewis Research, Inc. / Foothill Family Clinic
Salt Lake City, Utah, United States, 84109
J. Lewis Research, Inc. / Foothill Family Clinic South
Salt Lake City, Utah, United States, 84121
United States, Virginia
Clinical Alliance for Research & Education – Infectious Diseases, LLC (CARE-ID)
Annandale, Virginia, United States, 22003
Virginia Research Center LLC
Midlothian, Virginia, United States, 23114
United States, Washington
Benaroya Research Institute at Virginia Mason
Seattle, Washington, United States, 98101
Wenatchee Valley Hospital
Wenatchee, Washington, United States, 98801
Argentina
Hospital Militar Central Cirujano Mayor Dr. Cosme Argerich
Caba, Argentina, 1426
Brazil
Hospital Santo Antonio/ Associacao Obras Sociais Irma Dulce
Salvador, BA, Brazil, 40415-006
CEPIC – Centro Paulista de Investigacao Clinica e Servicos Medicos Ltda (Casa Branca)
Sao Paulo, Brazil, 04266-010
Germany
CRS Clinical Research Services Berlin GmbH
Berlin, Germany, 13353
Medizentrum Essen Borbeck
Essen, Germany, 45355
IKF Pneumologie GmbH & Co KG
Frankfurt am Main, Germany, 60596
Universitätsklinikum Hamburg-Eppendorf
Hamburg, Germany, 20359
CRS Clinical Research Services Mannheim GmbH
Mannheim, Germany, 68167
Studienzentrum Brinkum Dr. Lars Pohlmeier und Torsten Drescher
Stuhr, Germany, 28816
South Africa
Newtown Clinical Research Centre
Johannesburg, Gauteng, South Africa, 2113
Jongaie Research
Pretoria, Gauteng, South Africa, 0183
Limpopo Clinical Research Initiative
Thabazimbi, Limpopo, South Africa, 0380
Tiervlei Trial Centre, Basement Level, Karl Bremer Hospital
Cape Town, Western CAPE, South Africa, 7530
Turkey
Ankara Universitesi Tip Fakultesi, Ibni Sina Hastanesi
Ankara, Turkey, 06230
Hacettepe Universitesi Tip Fakultesi
Ankara, Turkey, 06230
Istanbul Yedikule Gogus Hastaliklari ve Gogus Cerrahisi Egitim Arastirma Hastanesi
Istanbul, Turkey, 34020
Istanbul Universitesi Istanbul Tip Fakultesi
Istanbul, Turkey, 34093
Istanbul Universitesi-Cerrahpasa, Cerrahpasa Tip Fakultesi
Istanbul, Turkey, 34098
Medipol Mega Universite Hastanesi
Istanbul, Turkey, 34214
Acibadem Atakent Hastanesi
Istanbul, Turkey, 34303
Kocaeli Universitesi Tip Fakultesi
Kocaeli, Turkey, 41380
Sakarya Universitesi Egitim ve Arastirma Hastanesi
Sakarya, Turkey, 54100
Thanks AP_Robert. I would add that Pfizer has been cooperating with the US Warp Speed distribution program, and the responsible military logistics team. The leading general has said that Pfizer has a good plan and he is ready for them to implement it, under his oversight.
McKesson has the major contract for distribution in the US because they distribute the flu vaccine. But he welcomed Pfizer as a parallel effort to handle the more demanding needs of their vaccine.
All of course depending on the results of the trials, for the Moderna, Pfizer, and other vaccine candidates.
The Covid-19 vaccine dilemma is far from being certified as Safe for Human use. Between the Asta Zeneca, Johnson, Pfizer, Sputnik V, and other in the trail process, as well as China which are at the last 3 stage test, but which been found very effective.
Scot, you are right in projecting a much longer recovery for thee airlines when the vaccines, wherever their origins, will take much longer to register thus loner positive impact of the Airlines. These delicate Human, presumptive curative vaccines, in a recent 60 Minute show, at least in the US military, who already have their Stockpile reserved to start Jabbing Americans throughout the country. Sounds very suspicious which of these vaccines will be used, and if the FDA, emergency or not have the right to massively oppressive these through the Military. Watch the 60 Minute show, an come to your own conclusions.
If the Chinese vaccine is as effective as is being touted, then Chinese airlines should not be reticent about sending personnel to Toulouse to pick up new planes…right? After all, the vaccine is already being administered to paying public in a test-case Chinese city (Jiaxing), so it’s a simple matter of ordering some doses for the people going to Toulouse…right?
And, yet, there are no Chinese coming to Toulouse. I wonder why?
China’s Sinovac vaccine trial halted in Brazil
https://www.bbc.co.uk/news/world-asia-china-54883383
Well, well, isn’t that interesting.
It won’t be the last time that we hear news like this…for lots of different candidate vaccines…
@Bryce:
From AP: ‘Brazil’s health regulator has halted clinical trials of the potential coronavirus vaccine CoronaVac, citing an “adverse, serious event.”
Adversaries of President Jair Bolsonaro said they feared the decision — posted Monday night on Anvisa’s website — was motivated not by science but by the leader’s political hostility to the country and state involved in producing the vaccine candidate.’
One is not called “Trump of the tropics” for no reason.
Link: https://apnews.com/article/virus-outbreak-brazil-health-clinical-trials-sao-paulo-cfe15d9de3909eb58d08e39363aa0786
From Dow Jones: Brazil to resume trials of China’s vaccine – it’s safe to continue the tests
Thank you, Pedro.
@ Pedro
Great!
Any idea what the Chinese are paying the participants in the Brazilian Phase 3 trials?
And/or if Brazil has been promised a batch of the vaccine if it gets approved?
You’d wonder why they’re even bothering with the phase 3 trials in Brazil when the vaccine is already being administered en masse in China. Probably just so as to satisfy “western protocol”.
https://www.latimes.com/world-nation/story/2020-10-29/china-coronavirus-covid-19-vaccine-secret
Still interesting that, despite this vaccine, Chinese airline workers are “afraid” to visit Toulouse.
Reporting is that Brazil offered to conduct the Phase 3 trials in partial exchange for rights to produce the vaccine in Brazil.
They are also assisting AstraZeneca with a Phase 3 trial in Brazil, with a similar deal for production materials and rights in Brazil.
That was the quickest way for them to procure the vaccines. I’m sure they also want to ensure safety for the population.
@Pedro
I’ve since discovered (at least one reason) why China is conducting Phase 3 trials in countries outside of China: it’s because Phase 3 trials require participants to get infected…but there’s no (known) community occurrence of virus in China to cause such infection. It therefore has to be conducted in countries in which the virus is circulating…unless one wants to resort to deliberately infecting domestic participants. Of course, one can only guess what might be happening in domestic detention centers…
Very different development paths for Chinese and Russian vaccines, as opposed to the West. No Western vaccine can be approved without Phase 3 trial results.
Also halting of a clinical trial is routine for any adverse result, until it’s understood. Others have been halted as well, then resumed once the cause is identified as being unrelated to the vaccine. But ethics require that to be positively determined before proceeding.
The anti-vaxxers generally post the halt, but not the resumption that follows. That’s the “outlier science” selectivity in action.
>>> If the Chinese vaccine is as effective as is being touted, then Chinese airlines should not be reticent about sending personnel to Toulouse to pick up new planes…right? <<<
Bryce,
I think you made that up. Got a link?
Hard to reply to a comment like this when you haven’t taken the trouble to specify what you mean by “that”; after all, the text that you quoted contains two sub-sentences.
But the following link may satisfy your itch:
https://www.cnbc.com/2020/11/07/chinese-airlines-are-shunning-some-deliveries-of-airbus-aircraft-citing-pandemic-reuters-citing-sources.html
Note, in particular, text such as:
“Chinese airlines are shunning some deliveries of Airbus aircraft, citing fears of coronavirus infection for their staff in the latest tussle over efforts to keep delayed deliveries on track despite the pandemic, industry sources said”.
Norm:
For better or worse, the US Military will force vaccination on their own people if they deem it necessarily. You join the US Military and you sign up for that as well – its part of and legal agreement.
It has nothing to do with vaccinating the citizens.
According to this article, less than 20% of the worlds population had ever flown in 2017.
https://www.cnbc.com/2017/12/07/boeing-ceo-80-percent-of-people-never-flown-for-us-that-means-growth.html
World’s population is 7 bn, 20% of which is 1.4 bn. The 1.5 bn doses would be enough to cover this. It is not difficult to suspect the population who is flying is richer and more likely to get a vaccine.
You also dont need to get everyone vaccinated in 2021 to have traffic levels back up by 2023-2024.
Does not matter. That 7% crosses with the 93% and then move it onto the non travelers (which is how it spread)
So yes you do need herd immunity to get travel back.
Airlines are staffed by non travelers as well as fuel, parts, you name it.
It seems that Michael O’Leary at Ryanair doesn’t grasp the complexities of the vaccine landscape:
“Vaccines mean summer could see 80% of 2019 demand: Ryanair chief”
https://www.flightglobal.com/strategy/vaccines-mean-summer-could-see-80-of-2019-demand-ryanair-chief/141057.article
More news: AerCap cancelled another 24 MAXs in Q3 (Dutch article):
https://luchtvaartnieuws.nl/nieuws/categorie/2/airlines/leasemaatschappij-aercap-wil-nog-minder-boeing-737-maxen
No one does, this is not a normal event or any history to go with it.
In the current situation I think most lessors would cancel orders if they could in general. Might be better to offer leasebacks from the start and don’t have to pay Pre Delivery Payments, which don’t generate profit.
Sorry, I know it’s off topic.
EU bought 300m Biontec vaccine doses, that might be good for 150m people. But EU has much more people, so many people will never get a vaccine. There might be 10 doses kept for each politician.
Testing is reduced now because of capacity restrictions in Germany. So people who had contact to an infected person won’t be tested if they don’t have symptoms. But for professional soccer players and politicians there are no restrictions. This smells ugly.
As regards your vaccine comment:
– Even if they wanted more doses, they couldn’t get them at the moment, because other countries are also buying up large numbers of doses. The real fun starts when the doses actually have to be distributed…who *actually* decides the allocation that occurs? Nobody (except Rob, perhaps) buys the story of an independent body that will administer this.
– Doses for 150m people is sufficient for a first round…that equates to a third of the population of the EU, and is enough to vaccinate the vulnerable and the medical profession. Contrary to the situation in the US, people under 40 (about half the population) essentially run zero risk from this virus, so they can wait for their jab until 2022. People in the range 40-55 have low risk.
https://ec.europa.eu/eurostat/statistics-explained/index.php/Being_young_in_Europe_today_-_demographic_trends
https://www.statista.com/statistics/1105512/coronavirus-covid-19-deaths-by-gender-germany/
– Then comes the really interesting bit: the EU has also bought large doses of other candidate vaccines (with production in Europe), e.g. the Moderna one. So, in principle, if those vaccines also “come online”, there’d be enough to vaccinate a far greater number of people in the coming year. But, as commented w.r.t. earlier articles, this issue is fraught with difficulty and thorny complications.
– Plus: with the infection rates currently in the EU, every day is a small step closer to (temporary) immunization via infection. Remember that the actual infection numbers are conventionally considered to be about 15 times higher than the official numbers, due to a combination of factors (non-testing of asymptomatic infectees, at least 20% false negative of PCR test, not everybody with symptoms presents for testing). We’re currently just under 10 million official cases in the EU, which translates to 150 million probable cases — a third of the population.
The US expects to have 700 million doses by summer 2021 (CDC and NIH, as per Redfield and Fauci). Other western countries will have enough doses on hand by then for their populations as well. The issue will not be availability so much as patient application. That could take until the end of the year, or longer.
The world should have enough doses by the end of 2021. But again application will be the major issue.
@Bryce, on dangerous thing is to assume the “risk” is the same as “risk of death”.
I personally know five people who have contracted COVID-19:
– two with no symptoms (one in 40s, on in 90s)
– one with coughing etc, not hospitalized (50s)
– one with serious symptoms, hospitalized (50s)
– one death (90s)
The fourth person on the list spent months in the ICU, including ventilator and dialysis. Seven months after infection, he is not able to return to work yet.
Non-fatal doesn’t necessarily mean it’s just like a flu.
@ Thysi
I can also draw up a list like that (11 in total), although nobody on my list ended up in an ICU, and only one (in his 80s) ended up in hospital for a week on O2. But I don’t really understand your point. Are you trying to point out that people in their 50s are at risk of ending up in hospital with this? Absolutely! But don’t forget to compile statistics for all the other conditions that can put people in their 50s in hospital, and then compare relative sizes of those statistical groups.
Remember that getting your appendix removed will put you in hospital, for example. As will mononucleosis, Lyme, hepatitis, legionella, severe allergic reaction, severe autoimmune conditions, sepsis, kidney stones…the list is endless. And don’t forget severe flu. I had a 55 year-old colleague who died of flu!
I think Thysi’s point was that the morbidity of COVID is greater than the flu, which is true.
Comparisons to the flu may seem more valid within certain age groups, but the data show that the breakpoint appears at age 15, Below that, flu causes more deaths, above that COVID does.
https://freopp.org/comparing-the-risk-of-death-from-covid-19-vs-influenza-by-age-d33a1c76c198
The rate of severe but non-fatal illness also roughly tracks the morbidity levels. And the risk of lasting organ damage after illness is greater with COVID than the flu.
Nor do you know if its setting you up for a stroke no matter how recovered you are.
There are indicators of long term health impact.
You can’t cherry pick data and say its relevant.
We do know there are 100s of thousand of deaths in the US alone.
Yes some were on their last lap and some had many years left.
20 years from now we will know the true impact.
@Bryce, my data points are anecdotal and are not intended to prove anything — except to show an example of severe health impacts AFTER the COVID-19 infection, considerably more than could be expected from a severe flu. I have seen other similar long-term impacts in my reading, too, although I have no references handy.
So, my point is that the mortality rate does not capture all of the risk, long-term health issues exist and more may yet be discovered as more time passes since the start of the pandemic.
@thysi
“long-term health issues exist”
That applies to a whole scala of situations…including something as simple as pregnancy. It also applies to substance abuse, for example, which is essentially omnipresent and includes use of tobacco and/or alcohol. And don’t forget all the medical misery caused by obesity, including diabetes and heart disease.
With regard to the much-hyped “long CoViD”, the following link has become somewhat of a reference. Note the sentence “1 in 20 people with Covid-19 are likely to suffer symptoms for at least eight weeks.”
https://www.kcl.ac.uk/news/study-identifies-those-most-risk-long-covid
And before running out to ring the church bells, check first how many other conditions produce post-viral fatigue…including relatively common ones such as mononucleosis, hepatitis and herpes zoster.
The WHO estimates that 10 percent of the world population has already had CoViD. In parts of Europe, the figure is probably closer to 30%. Do you really think that there are tens of millions of people here that are hobbling wrecks?
So again, the issue (as correctly raised by Thysi) is the severity of the effects on the people who have increased vulnerability.
Some of these have become the so-called “long-haulers”. They cannot be dismissed simply by pointing to the larger subset of people who have mild or asymptomatic infections.
Here is a Nature article which documents some of those effects. Notably since COVID is new, this research is just now getting started. If this kind of illness can be avoided by vaccination, then we have an ethical and moral duty to try.
https://www.nature.com/articles/d41586-020-02598-6
We also know that permanent damage leads to chronic conditions later in life. So for some, the true consequences may not be fully understood for years.
On Reuters:
More MAX order losses for Boeing in October, and continuing 787 quality issues.
https://www.reuters.com/article/aerospace-defense/idUSKBN27Q2IP?il=0
In October Boeing deliverred only four 787.
If they are still at production rate 10 per month, Boeing couldn’t fix the tail issues for 7 months.
Are you surprised?
We’re starting to see a flurry of cancellations, and — regrettably — it’s only a matter of time before we see more airlines going belly-up. This is not a good situation for BCA to be in.
The solution? Turn yourself into an aviation “K Mart”, start trying to sell MAXs at bargain basement prices, and hope that the meager margin that you make here and there will be enough to ward off having to go to the soup kitchen.
How low the mighty have fallen.
Who wouldn’t be surprised that Boeing can’t build planes to their own specs. It seems the four deliverred last month were just luck not skill, as if they don’t know how to do it.
If they have over 50 B787 parked with tail issues it takes time. Out of spec stabilzers can’t be recycled, only replaced. But first they need a coach who knows how to do it and it seems they don’t have one.
I thought knowing that they made mistakes is enough, just fix it, but they can’t. Unbelievable
There might be other issues we don’t know about yet.
The stabilizer repair was described in the reporting. The two sections are unfastened, then re-clamped with the correct force and spacers and re-fastened. It takes time but they will catch up.
They had 50 aircraft in storage before the problems were discovered, so not all of those are affected, nor would they be delivered after repair, until the airlines are ready for them.
@Rob: According to Reuters report, Boeing identified the problem in February but did not disclose it until Sept.
Boeing’s financial report Oct 28:
787: Most of the inventory of 50 airplanes is heavily weighted toward quality control and rework, not a lack of demand, said Smith. Deliveries will pick up in 2021.
Few could be white tails but most have quality issues. The last 7 months 46 B787 were not deliverred.
Emirates recently asked to defer 777X orders to 787 because of delays and Boeing didn’t like it because they can’t even keep their 787 delivery schedule they have.
Estimate that 200 787 will need fixed world wide.
That would be having one or the other issue not both.
The good news is that this RNA-based vaccine is likely to be produced in large numbers, larger than many other type of vaccines. No matter how the situation develops, starting spring/summer 2021, we will have:
– way more people being immune (either vaccinated or through infection)
– better ways to treat ill people (mortality dropped by ~50% since the early days through better understanding – despite having no real drug)
– behavior modification, while this is not very reliable
So the prognosis by MoL sounds not complety absurd, yet it probably is the upper end of the spread of possibilies.
Actually, we have all three of the points you mention right now, when compared to March. And yet, despite that fact, the aviation industry is slowly slipping into the abyss, with no tangible improvement in sight.
By the timeframe that O’Leary mentions, we’ll have enough of this vaccine to have vaccinated 5% of the population. I don’t see how such a low percentage is going to change policies with regard to quarantining. According to current WHO estimates, at least 10% of the world population has had CoViD, but that hasn’t helped to ease quarantining requirements. What difference does an extra 5% make?
I do agree with you that, by the timeframe O’Leary mentions, a far greater percentage of the population will have had CoViD, and will thus have initiated some form of immune response. But his comments referred specifically to the vaccine situation.
There are 6 or 8 viable Western candidates that use the same idea.
All are gearing up for production. So its not just on one, the other may pass muster and you have multiple paths.
We just don’t know and that is all they should be saying.
Hell space Aliens may land and eat us all and out the window it all goes.
In U.S., the picture from those on the front line looks rather grim, cases are doubling, inceasing hospitalization is going to crush the health system and death rate will jump. Going to be a winter many would rather forget.
We had a similar situation in The Netherlands a few weeks ago. A small tweek of the restrictions knob* has caused our new case numbers to plummet, and hospitalizion/ICU occupancy is now also decreasing.
Even if the sitting US president doesn’t take similar action, there’s nothing stopping (Democrat) governors from taking their own steps at state level, is there? Now that Biden has set up a CoViD task force, he can basically just copy/paste similar measures onto his website, can’t he?
* Actions taken:
– Bars and restaurants closed (for 6 weeks), apart from takeout.
– Wearing of face masks “strongly advised” in indoor public spaces (not mandatory).
– Team sports suspended for all ages, with the exception of Premier League football.
– A week ago, an additional two-week closure of cinemas, theaters, museums and zoos was stipulated.
https://virusncov.com/covid-statistics/netherlands
OTOH “North Dakota hospitals at 100% capacity,
Gov. Burgum announces COVID-positive nurses can stay at work”
Bryce:
Sadly over half our states have Republican governors. Probably half of those are deniers.
Our Governor is pathetic. The City has taken far stronger measures.
Good news is he is up for recall, bad news is the Lt Gov is also pathetic.
The tough thing in the US is you had the federal government actively altering the message of the health agencies, for political reasons. That did a lot of damage, as it pitted the authority of the chief executive against the public scientists and servants who had responsibility for that message.
The message should have been unified, but alas, was not. It clearly divided the country and created a deficit of public trust. That needs to be made up now by the new administration.
One thing that may help, is the refusal to concede and the rejection of false positions by the courts. That should bring the true nature of the perpetrators into focus. But there is still a lot of trust that must be reestablished as well.
Rob: (yes I know this gets political) – this is where I think you always are off base. Like Bryce, you take selective data sets and impose it on reality.
I have zero faith that the new administration can overcome the issues we see.
Factually, those in the Repub party that are supposed to be responsible are outrageously not responsible and are not paying a price.
Like Boeing management (and others) unless they are punished, they will keep doing the same thing until forced into another patch.
The same conspiracy side keeps electing the same ones that enabled a historically ugly and worst administration in our history by leaps and bounds.
Ironically, the only thing that saved us is our fractures state election system (50 separate ones)
Unlike Belarus and the rest of the world there is no Federal (central election) Control so each of the 50 states has to be compromised (or at least the swing states) to corrupt the process entirely.
Ergo, its not that they would not have done it, they simply could not. They violated every law and ethics on the books though in to the Govt power to try to sway it and still are.
Keep in mind, McConnels pledge in 2008 was to make Obama a one term president. Guess who is still in DC obstructing anything positive?
Will things be better? Yes. But you have all those tin pot dictator enablers that are not going away.
Ergo, the reality of facts says otherwise.
TW, I cannot say what will happen, I was just expressing my hopes for improvement.
Everything depends on what both sides choose to make of this opportunity. It’s really their choice But I think it’s clear that neither side has the power to ignore the other, so they have to work together on some level.
I do agree with you about the independence of the state/county electoral system, it is a saving grace of our democracy.
For those who may be open-minded and wish to acquire a better understanding of the vaccine development process, I’d recommend this blog. The author has a Ph.D in organic chemistry and is well versed in clinical trials and the FDA approval process. It’s highly technical, detailed, and informative, but is written in easily understood terms.
https://blogs.sciencemag.org/pipeline/
There are numerous entries for COVID, including this week’s on the Pfizer announcement. Also there is an excellent entry from October on immunity, as well as from September on the trial protocols and how they work.
I have learned a great deal from this site, so maybe others here can as well. It’s an independent & balanced viewpoint from someone experienced in the industry.
Rob:
Thank you for the link. I will watch it and see what I think of it.
This looks good but have not drilled down yet.
Rob:
I read the first article that was on the T cells. Phewee, I would rather troubleshoot an automatic transfer switch !
Good thing he sums things up.
My first take is very positive on the site. T cells have had all too little research (and the research I have done has been of no help)
It does confirm what I thought though and that is immunity and aniti bodies with the T cells and the types of T cells is not understood and its a shock in this day and age for the pretty shallow push on anti bodies with there is a whole universe of body response ignored.
Have to wonder if the corporate push wants easy vs getting a full understanding as long as it works.
So far this guy checks out as spot on and very good support.
Into the third article (this one on Alziehmers) and his assessment meshed with the other critial assessments I have read on that subject of what Biogen is trying to pull.
Unfortunate i as it also shows why people don’t trust corporation (let alone politicians) . Scams like Biogen are trying to pull off makes it valid to question all corporations as their move is more the norm.
With Pfizer, it may have been pre- done (and I caution the different between legal and ethical ) , but the Optics are bad leading to a reinforcement of public disbelief.
Or as has been stated, just because you are paranoid does not mean they arn’t after you.
WN is said to be in talk of 737 MAX “white tails”. However, any deliveries would replace similar number of existing orders.
On the joint subject of vaccines and aviation, has anyone else noticed the total lack of any cogent effort to close off movement of persons from Denmark? Despite strong indications that the new (mink-associated) variant has a very different spike protein to existing variants, and the fact that a Danish minister described the situation as “very, very serious”, to date only the UK has made any attempt to close its borders to movements from Denmark (as well as a half-baked “self quarantine” move by Ireland). It seems that the EU/US haven’t learned much since the virus escaped from China back in January.
The ECDC is “evaluating the data”, and there’s a stony silence from authorities in other countries. In other words: do nothing while the horse bolts, and then lament that you made no attempt to close the stable door. You’d have thought that, where CoViD is concerned, one would have learned to “shoot first and ask questions later”.
That’s the different between a lab nerd and a crisis manager.
https://www.ecdc.europa.eu/en/news-events/ecdc-assess-risk-associated-spread-sars-cov-2-mink-farms
https://www.theguardian.com/environment/2020/nov/05/danish-covid-19-mink-variant-could-spark-new-pandemic-scientists-warn?ref=upstract.com&curator=upstract.com
@Bryce
https://www.theguardian.com/environment/2020/nov/09/denmark-drops-plans-for-mass-mink-cull-after-covid-mutation-fears
The Guardian in England reported that political opposition in Denmark had halted the cull, for the moment only perhaps
It appears ‘the authorities’ have been aware of the mink infections for some time : yet denied there was any ‘problem’, and of course zero debate : have yet to publish more than a Press Release as per Pfizer and have not released ‘date’ to scientific institutions
As you say the rest of Europe = no comment
It is curious to observe this kind of absolution authoritarianism coupled with absolute nationalism in what some would consider, perhaps wrongly, an exemplary EU country
Makes one a tad forgiving for the outrageously stupid and ineffective authoritarianism of a Boris or a Trump
@Gerrard White
Yes, I already read that the mink cull had been stopped: unbelievable.
The Danish site in the link below gives lots of news on this topic. From the embedded tweet in the link (for example) you can see that vital genome data has been / is being withheld from broad release to the scientific community. An almost exact parallel to the attempted cover-up / fumbling that went on in China after the initial incidents at the wet market in Wuhan. It was bad enough that the EU made no attempt to close its borders in February, but it’s absolutely surreal that something similar is now happening within its borders, with no lessons learned. As if “asking” residents of Northern Denmark to stay within their communities is an adequate response. The policy here should be to seal off Denmark immediately, then analyze the data, and then re-open the borders if it is decided that the matter is a false alarm. I’ve since discovered that an expert on CNN (Amanpour) yesterday evening espressed similar disbelief that the borders were still open.
https://www.thelocal.dk/20201108/scientists-call-for-calm-over-mutant-mink-coronavirus
I’m wondering which country in the world will be first to put an army field marshall in charge of covid policy. We badly need that. Nerds can provide background advice, but they should not be determining policy. We discovered that back in NL in May, and things are now running more smoothly since. The old situation was that the nerds told administrators what path to follow; the new situation is that the administrators define the path that they’d like to follow, and they tell the nerds to come up with options that can facilitate that. A far more effective situation.
@Gerrard White:
Two corrections : ‘absolute authoritarianism’, and releasing ‘data’ not a date
There is debate over how dangerous the mink mutations would be to humans, or having significant resistance to a vaccine, given that the mink strain originated in humans.
This is different from the case of COVID coming from bats originally and being mutated through the pangolin. Some virologists have said it’s not likely to be much different after a single generation pass through the mink population. They say it takes a lot more than that.
I don’t know the answer here, just pointing out that there are varying views and the cull is a drastic non-reversible action, with perhaps not solid basis.
After the announcement by Pfizer yesterday, it appears that a game of “me too” has started among vaccine makers: Russia is now announcing that its Sputnik V vaccine is 92% effective:
https://www.reuters.com/article/us-health-coronavirus-russia-vaccine/russia-says-its-sputnik-v-covid-19-vaccine-is-92-effective-idUSKBN27R0Z6
An interesting allegation, seeing as the vaccine uses two human adenovirus vectors (Ad26,Ad5) to which there is considerable immunity in Europe.
Any takers?
These are all interim results. The Russian results were after 20 infections, which would not be considered statistically sufficient for a western Phase 3 trial. But as long as the trials continue and we see published data along the way, and especially at the end, they can be evaluated fairly.
At Pfizer, the team wanted to un-blind the interim results at 32 infections, but after consultations with FDA, doubled that to 64 cases, out of statistical caution. By the time that level was expected to be reached, the COVID surge had produced 94 cases. It’s now likely they will reach the 164 case mark fairly soon.
It all comes down to public release and analysis of all the data, before EUA is considered awarded
@Bryce
A link which explains the underlying ideology of what I call the PTA class but which most design as the PMC, and which you, I think!, call the nerds
Which class is most visible in the US but may be seen across the EU – this narrow ideology can or might be taken for an explanation of the extreme limitations of current policies, as exemplified in the Danish ‘mink’ situation and the lack of any responsible or reasoned response by EU authorities
https://benjaminstudebaker.com/2020/09/28/the-rump-professional-class-and-its-fallen-counterpart/
@ Gerrard White
For me, it’s not necessarily a class issue…although that may an underlying aspect. Instead, I cringe at the idea of asking lab nerds to suddenly assume the mantle of a crisis manager and strategist: they may know lots about DNA, but they know nothing about situation control. They’re far better in an advisory role than in an executive role. But, unfortunately, the average administrator feels out of his depth in the current situation, and prefers to *defer* to the nerds instead of purely using them to supply technical information on a per-situation basis. Even virologists at the helm of national bodies have very limited organizational experience, and have zero experience managing something of this magnitude. Luckily, that shortcoming was recognized in NL a few months ago, and has since been corrected. Some examples:
– In March, the nerds were telling the government for weeks that test capacity couldn’t be expanded, because of a shortage of test chemicals. The government turned the matter over to an ex-director of a biotech company, and it was solved within 10 days.
– For months, the nerds were saying that rapid tests were unreliable. So the government turned the matter over to a state research consultancy, which developed its own test, conducted tests in parallel with PCR tests to assess reliability, and concluded that the rapid test was in fact just as reliable as a PCR test (slightly better, in fact). The army is now being used to set up XL rapid test centers, in parallel to the regular test centers.
– The chief nerd still hasn’t convinced himself that face coverings work: he’s the type that won’t accept that today is Wednesday, because he hasn’t seen a peer-reviewed journal article in which that is proven. Luckily, the government started to ignore him on this point in May, first introducing mandatory masks in public transport, and subsequently advising broader mask use (becoming mandatory this month).
– The nerds advised an evening curfew 3 weeks ago as a means of decreasing case counts. The government told them to “get real”, and come with other options. Eventually, far less drastic measures were implemented, with excellent results.
So, is the picture a little clearer now? The basic tenet is: “A nerd is a good servant, but a bad master”.
@Bryce
I would add one element to your explanation of the strange influence of an hitherto discreet enough PMC subset
The PMCs, or the nerds, have made a power grab, because the administrative political and indeed academic classes were overwhelmed by their lack of understanding, preparation and panick
And made clear their need for cover – duly provided by the ‘follow the science’ crowd, most early and most notorious of which was the bloke from Imperial College, not an epidemiologist nor a virologist, but a ‘modeller’
It’s this segment that saw an opportunity – half way housers all of them, hop scotching from Pharma to Academy to Foundation to Administration, and back gain
In NL you say they have been put back in place – evidently not in US/UK, where they have thrown in with Pharma
@Gerrard White
Great point about the power grab.
The chief nerd here was starting to demonstrate a sickening level of vanity and megalomania…he viewed himself as something of a spin doctor.
Although I like Dr. Fauci, I also discern a certain media fetish where he’s concerned; I may be wrong, but I get the impression that he enjoys being in the limelight.
It will be interesting to see who’ll be calling the shots when the next US presidential term starts. Although Biden is willing to tackle the pandemic more proactively, he may be a bit too deferential to the expert committee that he’s assembling. It will be interesting to see how high the nerd factor of that committee is. I hope he puts a high-ranking military officer at the helm, to keep the nerds in tow.
Bryce:
Like Flyn in charge?
Careful of what you ask for, there are some real military nut cases.
Even the somewhat saner ones participated in a suppression of peaceful protests.
@Bryce
You’ll like this!
https://twitter.com/businessinsider/status/1326454622140174336
Pfizer’s CEO cashed out 60% of his stock on the same day the company unveiled the results of its COVID-19 vaccine trial – which comes first, the chicken or the egg
Pfizer say they are developing a powder form of vaccine, given the impossible logistics of their vaccine
@Gerrard White
What a gem!
I suspected on Monday that the SEC was going to be nosing around this issue, seeing as the press release was so out-of-the-blue.
On a similar note, the other Pharma in the consortium developing this vaccine (BioNTech) disclosed less-than-rosy Q3 results yesterday; when I saw the reports, I couldn’t help thinking that Monday’s press release was a distraction tactic.
https://www.fool.com/investing/2020/11/10/no-surprise-here-biontechs-q3-results-driven-by-it/
@Gerrard White
Thanks for the info on the powder form of the CoViD vaccine.
Here’s a link for others.
https://www.dailymail.co.uk/news/article-8936107/Pfizers-scientist-says-working-powder-form-COVID-19-vaccine.html
Perhaps someone from marketing, or an external consultant, told the nerds at Pfizer to “get real” and come up with something a little more workable? Pity they didn’t think of that earlier.
The logistics are not impossible, they simply are higher level which we can manage.
Better a vaccine at -80c than one in a developing powder.
Pfizer has an entire system setup to distribute the low temp one.
Kudos to a powder, but get the liquid now and through test and start paring Covd back if it works.
As for the CEO cash out, have to see if its legal and if he gets canned over it. Nothing new on CEO (but the CEO is not the vaccine either).
All their data is reviewed by independents.
I am not taking his word for if it works and no one else is either.
Certainly like Boeing, it should be illegal for shares to be part of the compensation, that is an integrity issue that is long over due to be addressed. .
This trade was done as part of a 10b5-1 trading plan, which have been created to prevent insider trading. The plan requires the price and date to be established in advance, in this case, on August 19. It includes other third-party safeguards as well.
Thus this exact same trade would have occurred whether or not the announcement was made on that day, and no profit was derived from the announcement.
Nice conspiracy theory, though.
@ Gerrard White
This article on CNN also discusses a suspicious stock transaction by Moderna executives last month. There have been calls for the SEC to investigate.
Regarding Pfizer: Bourla could have deferred the pre-scheduled stock sale – he knew about the coming press release a day beforehand. But he didn’t defer. Smells unsavory.
https://edition.cnn.com/2020/11/11/investing/pfizer-ceo-albert-bourla-stock-sale-vaccine/index.html
Bryce, no difference in his personal outcome if he did or didn’t defer. I suspect this allegation would have been leveled at any point after the stock rose. The SEC will dismiss these complaints as being without basis.
On the subject of the EU tariffs on Boeing products…Ryanair doesn’t expect to have to pay them.
https://www.reuters.com/article/us-ryanair-boeing/ryanair-would-not-expect-to-pay-boeing-tariffs-idUSKBN27R1CA
From the way it’s worded and previous Bloomberg report, would Boeing has to stomach the tariff to ensure delivery? Boeing’s grand strategy boomeranged, Again?
@Pedro The sales contracts typically require the operator has to pay the tariff. However, for customer relations, Boeing (or Airbus) may absorb the fee.
Thanks.
Link here https://www.bloomberg.com/news/articles/2020-11-09/eu-tariffs-on-u-s-made-jets-may-affect-ryanair-s-max-order
Just as Delta isn’t paying import tariffs (Airbus is), you can bet your Aunt Fanny that cheapskate O’Leary won’t, either.
Scott:
O Leary is just tight with a penny (or is that a farthing?)
Call him “Thrifty”.
Scott, there’s an irony of justice in that, if Boeing and Airbus each take the hits for their arguments before the WTO. Really points out how senseless this has become.
I hope things will change now and EU/US will reach a settlement that eliminates the tariffs. Each has been successful in eliminating the subsidy of the other. Time to bury the hatchet.
Rob:
The real irony really is at one time Boeing was not massive subsidized by government (all that hype about military contracts aside, for which they deliver the goods (well mostly and sort of)
On the other hand Airbus is and was both state subside and Germany, UK, France and Spanish subsided (Boeing is really only massively State subsidized until they abandoned the state doing it, well South Carolina of course but not quite the scale of Washington State ) .
then Boeing got to the corporate welfare trough and sucked up big time and arm twisting and threats etc (the usual line of doing business for US corporations now)
Its turned into a pot calling the kettle black.
WTO alwyas was corrupt and there alwyas has been the parcing and dicing or the so called rules and all the exceptions .
Might as well dump the whole thing, its all a joke.
WTO is just an employment agency for bad lawyers.
TransWorld “I had that discussion with a mfg over a new type compressor and while I needed the data, they sim,ply said, we have run it for 10,000 hours and that is all the time till now. Give us a year and we can tell you 18,000 hours. Its going to take 3 years to get a solid data on how long it lasts.”
That made me have a flight of fancy. When it comes to measuring life time for things like LED lights we have ways of accelerating the life tests, so that we can say it has a life of 10 years long before 10 years are up.
I wonder how much work is being done to accelerate drug testing. (Quite apart from the obvious ethical dilemma of giving some people placebo to see if they get the disease ! )
Ethical studies require trial members to acquire the virus naturally, unless there is a known remedy that can be administered. In that case people can volunteer to be purposely infected.
Since there is no remedy for COVID, we have to follow the natural course of infection, illness, resistance, and immunity. Then the various indicators of immunity can be measured within the body, but the exact mechanism by which they interact is not well understood.
We do know that a coordinated immune response is essential for COVID, and that serious cases are marked by lack of coordination. But again this is not well understood.
So research continues and we’ll learn more in time, but at present there is not a way to accelerate the determination of longevity of acquired immunity. The current clinical trials will help to establish that, by measuring the rate of decreasing indicators, but that will be an estimate. The true indicator of loss of immunity will be the statistical observance of re-infection within the population.
Robert W:
the problem is, taking the compressor, you can run it faster but you have to prove that running it faster does not change how fast it wears at normal speed.
The short answer is you can try, you may or may not succeed in speeding up the results and get projections.
RR only found out about its mess on the Trent 1000 after 5 years, then it had multiple issues. Their test setup was not real world so it did not show up.
Actually there are tests being done in the UK to deliberately infect people so they can accelerate the trials (volunteers)
They are using a placebo type to determine what kind of infection rate you need to ensure you get infected.
But again, its all volunteers who want to help the issue out.
Yes, that’s a “human challenge” trial, which were ruled out in the US, although Congress tried to encourage the FDA to allow them. China is reportedly doing it too.
Thanks, I am a mechanic and not medical so this is not an area I have the right terms for.
My gratitude to the people willing to do this for us.
I sure would not want to be a political prisoner in China!
@Bryce
This sort of dilemma is a social dilemma, solved by clever political understanding coupled with very high level administrative competence
The ‘science’ is used by one and all as a slogan, or as cover, or as a threat ‘or else’
And by Pfizer CEO Bourla to get rich quicker
Science is not a threat to those who are interested in truth & facts, only to those who seek to override them. If you follow the facts and the science, the worst case is you are proven to be mistaken, but then correction provides new opportunities. Refusal of correction only leads to greater error.
The Pfizer CEO thing is an excellent example.
Rob:
As an observation. You to do the same thing you call Bryce on.
Using our favorite example, when Boeing says we learned our lesson and all is well after a bit of corporate shuffling, you are not dealing with facts.
A statement is only factually in regards to the words. The results are not because there are no results.
Much like the vaccine, we cannot state 100% what the outcome is (you or me)
But we can go on what their track record is, which is all failure.
So then we get into analysis. If nothign changes that caused the failures, then the prediction is the failure will continue (and so they have)
A statement is not a fact of accomplished results.
Like the vaccine, you have to see if the statement (and the miner shuffling behind it) actually did accomplish anything.
At the core is cost cutting and missing quality and safety and that has not changed.
Unfortunately we have to wait to see, I can predict and back it up with facts of failure, but it is indeed a prediction (99.9% correct in my view)
Now if the board was removed, Independent members put on it, no more share buy back, no more Shares to management, no more bonus for doing your job, no more golden parachutes as well as a voluntary split of CEO and the Board Chiar (that was forced) ? That would be promising.
Return the ODA to FAA, also promising. None of it has occurred so you can be sure the failure of Boeing management will continue (lots of factual data to support that as well as all the factually data to show it continues downward if not complete changed what got you there in the first place)
Using Ford Auot as an example. Clay Ford tried to fix the company and failed. He finally brought in Mullaly who bargained into the position with full 100% support to change the whole company and its culture. That was a success. Prior to that Ford had reorganized endlessly and was in a death spiral because they never changed the structure that was the problem. You can’t trim the hedge, you have to rip it out.
So while I look forward to good information (and at times you do have it) insisting you are dealing with facts vs someone else, you fall woefully short in that regard when it comes to Boeing and Corporations (or what will happen under Biden) as you are indulging in wishful expressions not facts.
An interesting dichotomy of selective going with facts on Covd (pretty much spot on) and your defense of Boeing and the FAA.
@Gerrard White
Always interesting to see how irony-impaired people struggle with terms placed within quotation marks.
On the subject of impairment, I suspect that Mr. Bourla may be a little out of touch as regards how something appears vs. how it is intended. We may get some sort of fudge announcement in the next few days indicating that the transaction has been undone.
@Bryce
Regarding Pfizer and powder vaccine – I have no idea of whether it is a reasonable project, nor have read any comments concerning this
But it does seem clear Pfizer may be inventing a vaccine which may work as long as the very tough very expensive logistics can be solved and paid for by the…by someone else …and that that someone else is successful at persuading the US public to uptake, which success is rendered less likely by the corporate behaviour on display
The cold chain issue must have been clear from the start – Pfizer had done little work – ‘not our problem’
Carefully timing his Press Release, the CEO has taken his pay off before certification and logistics kick in to dampen enthusiasm impose some objective reality
This is typical Corporate take the money and run – Boeing Board and Pals took their money out before the results of their corporate failure became known
This degrading spectacle of corporate profiteering does little to encourage the people to the product, uptake on the Max may be no better than with the vaccine
But who knows – The FDA may turn out to have more teeth than the FAA
Just to address the inaccuracies here, the cost of distribution is included in the cost of the vaccine, and is being partially defrayed by the government in the US. The cold chain is partly why the Pfizer vaccine is among the higher priced vaccines at $40 per dose.
Second, the notion that Pfizer has left this as “not our problem” is completely false. They have worked from the beginning to develop the needed cold chain for manufacture and delivery, and have coordinated with the US Warp Speed logistics program to assure that roll-out will be both possible and successful in the US. My guess is that other countries using this vaccine have similar planning and coordination in place.
@Bryce
Please find link about recent FDA vaccine approval times, 2010-2020
https://jamanetwork.com/journals/jamainternalmedicine/fullarticle/2772943
Quote-
“Since 2010, most novel vaccines approved by the FDA required about 8 years of clinical development and were based on evidence from a median of 7 clinical trials, including at least 2 pivotal efficacy trials that were randomized, masked, and used a comparator group. These pivotal efficacy trials enrolled a median of 5000 patients, who were followed up for serious adverse events for at least 6 months. Given the urgency of developing a COVID-19 vaccine, trials will need to be larger than those supporting prior vaccine approvals and include sufficient follow-up time for emergence of adverse effects.”
It looks as though more and more criticism is being levelled at suspiciously speedy trialing – Pfizer PR is looking more and more suspect- no wonder Bourla took his money upfront
Again to be factual, the Phase 3 trials in the US have used much larger enrollments than normal so as to accomplish the needed level of rigor. Upwards of 2oK to 4oK, as opposed to smaller successive trials of 5k to 10k.
As we’ve discussed before, the acceleration in vaccine development has been on the front end in research, and on the back end in manufacturing. This is where the bulk of the 8 to 10 years of normal development time is spent.
The Phase 3 trials are being conducted to normal rigorous standards. Some minor acceleration in using larger single trials instead of smaller sequential, and in some cases, combining Phase 1 & 2 trials to save time. But there is no rush or desire to produce an unvetted or unsafe vaccine, at least in the west.
@Gerrard White
With this vaccine, the broad population essentially is the extended phase 3 trial group. As posted below in my link regarding Sinovac, hundreds of thousands of Chinese workers are being “encouraged” to take the local vaccine, even before phase 3 trials have ended. Anyone that gets a jab of a vaccine under an EUA is also, effectively, an extended phase 3 trial person.
Statistical base size is important! The phase 1/2 trials (72 persons) with the Pfizer vaccine candidate produced no serious side effects, but serious side effects did start to manifest themselves in the phase 3 trials (nominally 44,000 persons). In the case of the GSK Pandemrix H1N1 vaccine, incidences of narcolepsy only started to manifest themselves statistically once the vaccine was administered post-phase 3.
With regard to your comment about Bourla, you might turn out to be right. If, for example, the efficacy of the Pfizer vaccine is disappointing for the 65+ population, then that will be somewhat of a wet fire cracker…with attendant effect on share price.
The EUA specifically weighs the benefits vs the risks, to ensure the administration of the vaccine is safe and appropriate. The idea is to provide a quicker benefit if the determined risk is found to be sufficiently low, not to extend the trials so as to determine the risk.
The EUA criteria are posted online, they are pretty clear and straightforward.
@Bryce
Re the nerds and their vacant ‘follow the science’ slogan, please find the venerable Scientific American words of advice to the Biden transition team’s Covid plan
Quote
“The plan utilizes two phrases which arouse critical inquiry: a pledge to always “listen to science,” and the mischaracterization that public health “isn’t about politics.” It is dangerous to either “listen to science” unquestioningly or to think that a medical plan of this scope is not extremely political. Even though Trump seemed to ignore science entirely, science isn’t inherently good, and it’s certainly never any one thing. We can address COVID-19 with science, but science can sterilize an immigrant woman without her consent, and science can make an atomic bomb to kill hundreds of thousands. With a technocratic new administration, it’s important to be critical of the culture and politics of science.
Similarly, it would be dishonest to say politics has no role in health policy when health science is rigorously political. Who is being studied? Who is interpreting the data? Which populations are being tested? Who is receiving medications? Who is designing the studies, and how? These are all political questions.”
https://www.scientificamerican.com/article/we-finally-have-a-covid-strategy/
Blindly following the science has not been advocated here, and is a contradiction in terms. Science is by definition not blind, except where blinding fosters objectivity (as in blinded studies or blind justice).
The adjustment of science for political gain is a major problem, as we’ve seen in the US. All who seek to advocate for this have a political agenda, even Scientific American editorialists.
The larger question is how does politics, which operates under nebulous standards and rules, accommodate science, which is rule-bound by the physical world? It can be done, in the 60’s & 70’s with a less divisive culture, we passed the Clean Air and Clean Water acts with broad bipartisan support, and they were both resounding successes.
It’s notable that the Clean Water Act required presidential veto overrides in 1972 and 1987, but both measures passed overwhelmingly.
We could do that again now, but not if there are open attempts to undermine the common factual ground that science provides, for political ends.
@Gerrard White
Thank you…excellent!
Chimes perfectly with what you’ve been saying for weeks.
@Bryce
Thanks – the nerds will not give up easily – their position and income is unstable and under attack, their jobs being replaced by software, so will become extra shrill in an attempt to show their worth to their corporate masters, but their residual value, such as it is, is merely a nuisance value
@Bryce
Sorry – can’t be helped : two new links to show how the Pfizer shot is far from a done deal
To have Bloomberg publish such consistently skeptical articles does not look good for Pfizer on Wall Street, nor of course in the mainstream opinion of the American people
Consensus appears to be building that this Bourla payoff vaccine may be the wrong pony to back, because if it goes to scale in any way less than perfect it’s going to blow all chances of getting another vaccine accepted
Then run the software to see if there is a Plan C – emigrate to NZ or whatever billionaire safe house/panic room will have you
https://www.bloomberg.com/news/articles/2020-11-11/if-we-re-not-careful-a-vaccine-might-help-covid-19-spread
https://www.statnews.com/pharmalot/2020/11/10/harris-poll-covid19-vaccine-masks-distancing/
@Bryce Forgot to include the link :
Other contenders fast catching up Bourla’s pony on the back straight
https://www.fiercepharma.com/pharma/despite-pfizer-s-high-efficacy-expectations-other-covid-vaccines-may-have-a-logistics-edge
@Gerrard White
Thanks for the links. I had already seen the second one, but the first one was new for me. Of course, the underlying subject matter is not new, because it concerns the antibody vs. T-cell discussion.
On that note: in the link that I posted on the Sinovac vaccine, you can read why it’s reckless for the Chinese to already be administering mass doses of their vaccine: since the virus is not circulating in China (officially, at least), there’s no access to data regarding infected vaccinees, and it’s therefore not known what response the broader population will produce to the vaccine. It’s predominantly workers-for-export that are being vaccinated, so, in a disadvantageous scenario as described in your first link, they can indeed act as unwitting spreaders in the country to which they’re exported.
We should all note the old saying: “Fools rush in where angels fear to tread”.
@Gerrard White
With regard to the credo “follow the science”, have you any idea what “science” is actually being referred to?
There’s certainly huge science involved in vaccine development and test technology, but the US is already following those routes, so that can’t be what’s meant.
As regards social distancing, hand washing and face coverings: such measures have been practiced for hundreds of years, and fall more in the category of “common sense” and “basic hygiene” rather than “science”. Sure, you can use a stroboscope and high-speed camera to show that an aerosol from a sneeze can travel 6 meters in a subway car (that’s science), but putting on a mask falls into a totally different category. Farmers have been using face coverings to keep out smoke particles for centuries, if not millennia. And 16th century paintings show crowds keeping their distance from processions of lepers (with a bell ringer in front, to provide warning of approach). If that’s science, then so is opening a door…which, after all, involves statics, dynamics, acoustics and gas physics (air displacement).
Perhaps “follow the checklist”, or something like that, would be more appropriate. Or do you think, perhaps, that “follow the scientISTS” is what’s meant? A scary thought in view of our experiences here in NL.
@Gerrard White
Thanks for the extremely informative link from FiercePharma.
Interesting that the Pfizer vaccine is described as a “vaccine for the rich”, because regions such as Asia, Africa and South America are too far from the production centers (in the US and Europe) to allow feasible transport. Maybe Pfizer will start production on each continent? Although that still won’t help in road-less developing nations, unless fleets of bush planes are used. A logistical nightmare indeed!
At this rate, China will have ample opportunity to win over hearts in developing countries, since its vaccine does not have super-cold-storage issues.
It’s very welcome news that other vaccines will have interim results soon. No one manufacturer can carry the burden alone. Also each trial group will help us learn something about safety and side effects. Good efficacy numbers are expected for them as well, at least for the ones that use similar technologies.
Interesting that the Harris uptake poll says Americans won’t take the vaccine unless the infection risk is cut at least by half. That is also the limit set by the FDA, 50% efficacy. Same as the flu vaccine as well.
Fortunately we are looking at around 90% efficacy right now, which may or may not hold up or be reflected in other vaccines, but provides a very comfortable margin. Most Americans will accept that vaccine.
Regarding in Bryce’s post above: “Interesting that the Pfizer vaccine is described as a “vaccine for the rich”, because regions such as Asia, Africa and South America are too far from the production centers (in the US and Europe) to allow feasible transport.”
The following clinical sites in Argentina, Brazil, and South Africa, are among the 154 sites in the Pfizer-Biontech phase 3 COVID-19 vaccine study that has to date shown effectiveness in excess of 90%.
Argentina
Hospital Militar Central Cirujano Mayor Dr. Cosme Argerich
Caba, Argentina, 1426
Brazil
Hospital Santo Antonio/ Associacao Obras Sociais Irma Dulce
Salvador, BA, Brazil, 40415-006
CEPIC – Centro Paulista de Investigacao Clinica e Servicos Medicos Ltda (Casa Branca)
Sao Paulo, Brazil, 04266-010
South Africa
Newtown Clinical Research Centre
Johannesburg, Gauteng, South Africa, 2113
Jongaie Research
Pretoria, Gauteng, South Africa, 0183
Limpopo Clinical Research Initiative
Thabazimbi, Limpopo, South Africa, 0380
Tiervlei Trial Centre, Basement Level, Karl Bremer Hospital
Cape Town, Western CAPE, South Africa, 7530
https://clinicaltrials.gov/ct2/show/NCT04368728?recrs=a&cond=COVID-19+vaccine&cntry=US&draw=2&rank=8
@Bryce
As for the empty headed mantra ‘follow the science’ it is used as precisely that alone –the nerds can beat the poor deplorables over the head with their lack of education, and exploit a residual respect for big sounding words of ‘technique’, and counter their revolting tendance to indulge in religion of which ‘science’ is commonly taken as the enemy/antidote
It’s a point of survival for the PMC class to invent and PR such slogans in defence of their corporate masters – to put it the other way round, as far as corporate is concerned this slogan does little harm, lip service to ‘science’ is about all the faith they can tolerate
As you remark– very nearly every measure that may be taken with any degree of efficacity against a corona follows common sense
Every problem the US has run into is not only from lack of common sense, lack of ability to organise and administer common sense, and lack of willingness to apply it in their own lives
Common sense is a commodity which resists commerical exploitation, so….
As for the ‘science’ – this they sell, at least they want to sell it, if ever they could figure out some appropriate application of ‘science’ and how to sell it
And those ‘scientists’ often turn out not to be actual scientists but ‘modellers’ – ‘modellers’ are a step down from PR people because they not only make up conclusions they make up the facts, sorry the ‘data’, they claim to base their conclusions on
On the subject of vaccines:
An interesting article on the somewhat cowboy-like practices in China regarding the Sinovac vaccine.
https://www.latimes.com/world-nation/story/2020-10-29/china-coronavirus-covid-19-vaccine-secret
Pfizer’s so called distribution plan – get the Feds to do the job, and us their now infamous boxes, which do not work, or have not yet been shown to work
Links to MSM severe doubts in Health Care as to possible successful distribution of this vaccine
Pfizer is MIA
https://edition.cnn.com/2020/11/10/health/pfizer-vaccine-distribution-cold-chain/index.html
https://www.statnews.com/2020/11/11/rural-hospitals-cant-afford-freezers-to-store-pfizer-covid19-vaccine/
Absolutely untrue. Pfizer has been working with US Operation Warp Speed, as well as UPS, FedEx, and DHL. to develop the delivery network that precludes the need for special freezers at the destination.
General Perna has said he’s ready to distribute the Pfizer vaccine on 24 hour notice. UPS has opened new specialized freezer farms at their hubs in Louisville, US and Venlo, Netherlands. FedEx has 90 refrigerated storage facilities worldwide, which are being upgraded. DHL is upgrading worldwide as well, including a major center in Indianapolis, US.
Overall the goal is to deliver from a storage freezer location to the administer location, within a maximum of 3 days, leaving 5 days for use after transfer to local ordinary freezers. For locations that don’t have freezers, a repack of dry ice will also give 5 days for use.
In an example given for the Virgin Islands, the vaccine shipments from the US will be matched with dry ice shipments from Puerto Rico, so no freezers will be needed at the destination.
Pfizer has been heavily involved in all this. It’s a huge challenge and there will be learnings as they go for sure. It will start off with lower numbers and build with time. But to dismiss it out of hand, no, that’s just not truthful.
When asked about the success of this operation, General Perna said he’s confident he can deliver the vaccine, but what keeps him up at night, is the negative messaging that discourages people from wanting or trusting the vaccine.
So there will be a huge effort put forth to get the positive message across. If this all fails due to disinformation, that would be a national disgrace. As Perna said, in that case, shame on us.
Just as NZ and Australia were trying to set up a “travel bubble”, the business district in NZ has gone into lockdown again due to a mysterious CoViD infection in a female student. In the time interval between her test and the test result, she went to work, visited various eateries, took cabs, and shopped.
Again, this just goes to show the knife-edge that bubble countries are living on, and the incessant vigilance that is required. China had 129 mysterious infections in a factory near Kashgar last month…nobody knows where they came from.
One possibility: the virus can circulate freely for a long time if the infection chain only comprises asymptomatic persons. Unless periodic blanket testing is done — like in Singapore — such an asymptomatic chain won’t be detected until it produces a symptomatic person.
This is a periodic localized temporary lockdown, to capture and contain outbreak events, with small groups of infections numbering in the 1o’s. Meanwhile the other areas can carry on as normal, without the restrictions we are facing now, or the fear or reality of COVID-related illness, or death.
Compare this to thousands of infections per day, with the consequent illness and death to follow. Even though the rate of serious illness & death is only several percent, that’s still many lives lost or damaged per day, unnecessarily.
Apart from the two of you, I don’t know anyone who would choose the latter over the former.
@Bryce
Exactly, when you fail efficiently or rather safely to import men to do your fishing for you, you live in this perpetual tremble on the brink
Perpetual is the word is it not? If not permatesting and vaccining for all eternity – which could be said to be the worser fate?
The bug can ‘do’ minks and back – ‘doing’ sheep and back may take him awhile
Meanwhile he comes in on food or cold surfaces, or perhaps a seabird
@Gerrard White
Actually, in one of the links that I posted yesterday regarding the Denmark issue, it was stated that the virus can also potentially form a reservoir in animals related to the mink, e.g. ferrets, weasels, stoats and badgers. And there are plenty of them in the wild.
Regarding bubble countries: advocates of the bubble concept forget that the general population in non-bubble countries is building up immunity through exposure…so there’s a benefit in return for the death toll. And unlike a person vaccinated with a vaccine that only emulates a protein spike of the virus, someone infected with the virus itself is exposed to the full genetic package of the virus. That’s why the best vaccines use actual killed viruses, rather than just protein segments. Unfortunately, no such vaccine is forthcoming in the case of CoViD.
From a Nature paper regarding the benefit of mRNA vaccines:
https://www.nature.com/articles/nrd.2017.243
“The use of mRNA has several beneficial features over subunit, killed and live attenuated virus, as well as DNA-based vaccines. First, safety: as mRNA is a non-infectious, non-integrating platform, there is no potential risk of infection or insertional mutagenesis.”
(Impossible to contract COVID from the vaccine)
“Additionally, mRNA is degraded by normal cellular processes, and its in vivo half-life can be regulated through the use of various modifications and delivery methods. The inherent immunogenicity of the mRNA can be down-modulated to further increase the safety profile.”
(After provoking the desired immune response, the vaccine is assimilated by the body and does not linger as a live or weakened agent)
“Second, efficacy: various modifications make mRNA more stable and highly translatable. Efficient in vivo delivery can be achieved by formulating mRNA into carrier molecules, allowing rapid uptake and expression in the cytoplasm.”
(The vaccine generates a reliable immune response with fewer and less severe side effects)
“mRNA is the minimal genetic vector; therefore, anti-vector immunity is avoided, and mRNA vaccines can be administered repeatedly.”
(The vaccine is highly targeted and the body does not develop an immunity to the vaccine itself. The immunity response to the target can be repeatedly enhanced. For COVID, twice is enough)
“Third, production: mRNA vaccines have the potential for rapid, inexpensive and scalable manufacturing, mainly owing to the high yields of in vitro transcription reactions.”
(Replication can be done easily and quickly at large scale since no incubation is required for live virus)
Bottom line is that while there are advantages and disadvantages to each method, viral-loading vaccines are not “best”, mRNA vaccines have significant benefits, and allow solutions not available with viral-loading vaccines.
@Bryce
Thank you Bryce – there are all sorts of mink similar animals to act as reservoirs – I was deliberately harping on the ind ag food factory aspect as a potential reservoir, such factories are perfect breeding grounds for viruses, and are the soft unprotected underbelly of the US
I quite agree with you on ‘bubble’ countries, and then some : it can be seen that to practice the full panoply of measures, masking distancing, vaccining if ever, over a number of years, will involve such weakening of the local population immune systems as to render these people ‘naive’, as they will avoid –perhaps- this bug but also many or most of all related coronas and influenzas – within a short time to attain the kind of virgin status akin to those innocent’ populations the pockmarked scurvy mangy and infectious europeans discovered in 1492 –
The same problem you point out the Chinese face : and although the Chinese have a very disciplined population the already creaky (fisherman !) discipline on display in those anglo antipodes is unlikely to prove 100% efficient
The Pfizer pony is one legged already – ‘vaccine for the rich’ is indeed an unwinnable slogan, and the US ruling élite derive panick as well as profit from countering China – to let China gobble up the vaccination of the Third World while they have bet on a vaccine no one can take outside of the richest areas of their own country would be another Pyrrhic victory
So we shall see Bourla further sidelined, as Wall Street anticipated with his pay off- this was a useful clear the decks now we mean business style Press Release : over the next few months will be selected a more efficient as well as cheaper vaccine, a national ‘Big Western Science’ champion worthy of doing battle with the Russian and with the Chinese candidates
The US ruling class is at long last waking up to the fact that the US has lost a huge amount of world respect, power and influence so far in this crisis, to allow a vaccine victory to Russ/Chi would be the seal of defeat
@Gerrard White
I realized that you were poking fun at industrial animal husbandry…but you were making a valid point, seeing as sheep farming is an important industry in NZ. And sheep are, in fact, potentially susceptible to infection with CoViD….one of about 215 species that are now known to be potentially susceptible. If we’ve already discovered that minks can act as reservoirs for re-infection to humans, it’s probably only a matter of time before other animals are added to that list.
https://www.the-sun.com/lifestyle/tech/1583647/animals-pets-farm-zoo-coronavirus-covid-19/
It will be very interesting to see if researchers in NZ can ever pinpoint the source of domestic infection for that student in Auckland. No matter what the answer turns out to be, it will be worrisome.
I wonder if/when this will impact the extent to which flights from NZ are welcome in Australia…
@Bryce
Thank you for the information about sheep (and all the other species) being susceptible, I did not know this, and for the link
It just adds to NZ (and Aus) long list of potential woes – they may have stamped it out in humans, but may have to cull their sheep……..or face up to sporadic unexplained infections ? I suppose they can keep going, cull the cows and horses…rabbits…or hey why not test them all already ?
Perhaps, like the Danish with the mink, they have tested the sheep, perhaps they know the sources of the new infection, but they have not informed the outside world yet
NZ did a kind of bubble with the Aus, some of it one way only, and with only a few Aus states : looks more tokenistic than realistic
The US Department of Agriculture maintains an on-line list of all animals found to have been infected with COVID. There are cats, dogs, and minks, but no sheep or other grazing animals.
This is in the country with the greatest number of human infections in the world. New Zealand would be in a massively better position, having contained the virus to extremely low numbers of human infections.
@Gerrard White
Interesting link for you, detailing the pros and cons of various vaccine types.
https://nationalinterest.org/blog/reboot/pros-and-cons-different-covid-vaccine-technologies-explained-169291
Note a significant downside of mRNA vaccines:
“as they only allow a fragment of the virus to be made, they may prompt a poor protective immune response, meaning multiple boosters may be needed”
On the other hand, for live (weakened) virus vaccines:
“strong protection as vaccine mimics the natural infection process”
As expected, the “fast and easy” vaccines are coming online first, whereas the higher-quality ones are coming later:
“Several live-attenuated COVID-19 vaccine candidates are currently in preclinical trials”.
@Bryce
Thanks for the link
Wiser heads are coming to agree with you – Wall Street is coming to understand the need for administrative sophistication in waiving through the first very expensive vaccines in favour of a long term more effective vaccine, with a much higher revenue stream worldwide
The PMC nerd class is being informed and PR campaigns will soon be mounted
Wall Street wisdom is what got us in the various financial meltdown in the pass (care to remember 2008 and the wonderful prime mortgages?)
Or the famous, COSTCO is treating its employees too good, they need to gouge them (Boeing cowering workers model)
You can imagine (please) what I think about where higher revenue streams belong.
If they come up with better vaccines that is all to the good, in the meantime what is wrong with short term?
I have had booster shots for other diseases. I get a flu shot each year.
Its not exactly an insurmountable burden is it?
@TW
No one is saying Wall Street is good for anything but Wall Street, not even Wall Street
Like with Boeing, Wall Street calls the shots with Pharma; like with Boeing Wall Street makes the money, but the rest of the world gets second or third rate + crashes and many deaths
So with the bug – the Pfizer vaccine involves too much very expensive logistics even for many areas in the US, overseas it will not work
So Wall Street needs something else, something more saleable to scale
Setting up too many distribution systems is even more complex, they like to chose the winner, and even a slightly faulty, difficult to distribute, vaccine will scare off the other half of the US population not already scared off
The Pfizer vaccine will trot around forawhile in upscale use, it’s just a short term bet, the long term bets are not in yet
Gerrard, the evidence is contrary to this position. Within the US, distribution is essentially ready. It will be expanded to other countries as is feasible within the constraints of supply. As AP_Robert indicated, that list is also quite long.
In addition, other vaccines in the pipeline may ease the distribution burden. We don’t know the timing of that right now so are acting on the facts we have.
It would make no sense to stop the current efforts to wait for another, if the efficacy truly is around 90%. Just as it would make no sense to stop the other efforts, even with an efficacy of 90%.
Also any supply network that can deliver the most demanding cold chain, could also deliver less demanding vaccines. So putting those networks in place ahead of other vaccine arrival, is also a benefit.
@TW
I should add that Wall Street have their eye on the world market, local US distribution is a small and troublesome market, for which most opinion polls record little chance of significant uptake
Given the chaos and high degree of disorganisation so far on display in the US with regard addressing any aspect of this virus it seems remarkably unlikely that any kind of successful distribution and required % of uptake will be achieved
Wall Street is not indifferent to the advantage of a confused disrupted and desperate local workforce
Actually it seems very likely given the investment and planning that’s been done.
The most important factor will be the uptake rate, and that depends on defeating the negative messaging that tries to suppress it, along with suppressing the health and well-being of others. As I mentioned, a large effort will be put forward to provide the positive messaging that actually represents the truth.
The election has made that a little easier, as the priming and illusory truth that occurred, are now in the spotlight and are better understood. Social media and other public debate platforms are enhancing their ability to identify, highlight and combat disinformation.
That’s really all that’s needed, as when truthful information is provided, good decisions become far more likely.
Bryce, the conclusion regarding the fragment vs whole virus response issue of mRNA vaccines, was drawn by the authors of the article but is not listed in the original paper that was being quoted. Here is the link to original paper. The vaccine types are summarized in Table 2.
https://f1000research.com/articles/9-991/v1
With the National Interest publication, it’s always a good idea to check the source, as it’s mainly a blog and reprint site, not a journalistic or scientific site.
As I mentioned earlier, each type of vaccine has advantages and disadvantages, which are listed in the above table, as well as many other sources. But I have not seen any source suggesting that fragment response is a major concern in the development of mRNA vaccines.
The fact that other vaccine types, that have varying optimizations for application, will be coming forward is a very good thing, not a bad thing. And in no way does that detract from any success achieved the mRNA vaccines.
If the newer vaccines are judged to be superior, they will move to the forefront, as is proper. In the meantime, most countries will go with what is available to them.
@Bryce
As a vaccine seems to approach certification in the US, the usual idpol quarrels surface with
This was always likely to be the case, but hitherto disguised behind the language of front line essential and inessential, vulnerable and so on, anodyne categories that can be redefined by the hour
Now the racial issue is moving upfront and centre, and the usual suspects are already reaching for their lawyers
Given this kind of confusion is habitual in the US one is re assured, almost, for the clear warning that not only will the Americans not want to take this vaccine they will also quarrel about in which order and by or in which subgroup they will not take it
They have decided to argue about how not to distribute a vaccine before failing to do so
https://www.statnews.com/2020/11/09/health-experts-want-to-prioritize-people-of-color-for-covid19-vaccine-but-how-should-it-be-done/
@Gerrard White
Absolutely unbelievable.
But then, in the USA, a far greater susceptibility to CoViD complications is caused by excessive BMI than in other countries…and excessive BMIs are very prevalent among ethnic minorities. I was once in a supermarket in Kayenta (the main town in the Navajo nation) and I was stunned to see the number of obese and super-obese people around me…including children and adolescents. Couple that with a sedentary lifestyle and substance abuse problems and you get a CoViD tinderbox! A horrible situation for those people.
A fairer and more targeted distribution approach would be to put obesity high on the list of medical conditions warranting prioritized vaccination. After all, there’s no point in vaccinating thin Latinos at the expense of obese Caucasians, is there? But I suppose people will consider BMI to be privacy-sensitive personal information. Sigh…
Scary that this discussion is emerging in a country where firearm possession is widespread.
Gerrard, this is a discussion that needs to be had, but once again if driven by the science, it will be a fair outcome. The goal is to give the initial vaccine to the most vulnerable and at-risk populations.
We know pretty well at this point who those people are. So they will be prioritized. The government has plans for this as determined by the ACIP.
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/recommendations-process.html
Other frameworks exist as well, as listed at the above site, and all this will be reviewed by the incoming administration.
No reason to believe this is an insurmountable problem, it’s been considered and planned for a long time.
@Bryce
I agree that Americans in general are very unhealthy, are all fat and so on, the poorer more unhealthy than the rich, and so on
But to haul in racialism to provide a parallel sliding scale of deprivation by which health is to be adjusted for outcome of appearance is a surefire way of avoiding addressing the common overall and paralysing general nature of American poor health, and is in fact guaranteed to allow Americans to quarrel about the details while avoiding to address the reality of the catastrophic low level health they suffer from
The Africans in Africa suffer from robust good health as far as this particular virus is concerned, it is being American than is degrading and debasing for the health, not being African
As a principle of being, health would appear to address a commonality across a group which defies minute adjustments by the application of communal environments and régimes – basic equality : the group is healthy even if occasionally members are sick, and vaccines, as other treatments must be designed and applied with this perception and goal
Once exceptionalism or victimism deprives the notion of the group of any coherence and is merely a sounding board for dispute and division, divide and rule, then American health will continue to degrade at the speed remarked on over the last 50 years or more
You are right about the right to bear arms, so perhaps they’ll fight eachother to the death instead
@Gerrard White
Results published this morning in NL indicate that a significant percentage of older people do *not* want to get a CoViD vaccine as soon as one becomes available. More specifically:
– Aged 55-65: 55.1 %
– Aged 85+: 25 %
And that’s in a country with huge uptake of “normal” vaccines — except for a tiny minority of ultra-orthodox Calvinists who consider vaccination to be “contrary to God’s will”. A possible manifestation of the reservations about rushed vaccines. Remember than many members of that generation still have the Thalidomide disaster fresh in their memories. And they also remember he Narcolepsy issue in 2009.
So, whether or not one likes it, or can explain it, or can live with it or can solve it, sub-optimal uptake is going to be a fact.
Of course, on the other hand, if it transpires that vaccines have lackluster efficacy for older recipients, then it doesn’t really matter much if this age group has a low uptake.
One way or another: a headache for the normalization of aviation.
@Bryce
I am sure you have seen this report, but
https://www.reuters.com/article/health-coronavirus-russia-vaccine-idUSKBN27T0KO
It appears that the Russian vaccine Sputnik you have referred to is enjoying good sales, 1.2B doses ordered
Perhaps the orders for the Russian and the Chinese vaccines are outstripping the US – or is a tally not yet kept like of infections and deaths
If not it would be a good idea to put one up –
China 2.6B doses ordered; NZ 100M, Aus 200M and so on
Russia etc etc
@Bryce
Thanks for this report – I had no idea that there was such reluctance in the EU
The rush to get vaccines to market has back fired, if other EU countries share NL uptake reluctance in anything like the same %
So – who will all these vaccines be sold to?
Perhaps NZ and Aus will be takers, they’ll need a good stock – I can see little market in sub saharan Africa – Asia looks to go Russia China for their vaccines, which leaves South America?
Maybe we’ll get negative vaccine futures, just as we had negative oil
It’s all about the messaging, and early experience with the vaccine. Horror stories about medicine from 60 years ago, or isolated problems with a specific brand of vaccine, will raise uncertainty. Also the persistent notion that vaccines are not effective or will cause the disease.
However seeing the other half of the group taking the vaccine without issue, will be reassuring. So it will be a progression, but the needed percentage is likely to be achieved, with good results and truthful messaging.
@Gerrard White
Very interesting link about the South Korean production of the Sputnik V vaccine…thank you! South Korea is a highly developed society, so it’s very interesting to note their apparent confidence in the Russian product. Also, since endemic resistance to the vector viruses used in Sputnik V varies around the world, it’s possible that this vaccine will be very effective among Asian peoples. And, of course, no ultra-cold transport and storage issues.
Regarding the uptake in the EU: in general, people here are quite well-informed, so they don’t take their decisions lightly. They’re also able to make risk/benefit analyses, and realize that this virus is only posing a danger to a tiny niche group of the populace; despite the various “Frankenstein” stories doing the rounds, they personally know enough post-CoViD patients to realize that, outside the danger group, this disease essentially amounts to a flu. They’re not impressed by goblin stories of “maybe it will cause problems down the line”…just like they’re not hoarding supplies in case of an asteroid strike or nuclear war tomorrow. After all, exposure to sun, consumption of alcohol, or pregnancy can also “cause problems down the line”. The Dutch, in particular, have that attitude: they’ve been living below sea level for centuries, but aren’t awake at night worrying that the dikes will fail.
I agree with you that it would be informative to have a table of which countries have bought which vaccine.
@Bryce
The Koreans are very, very, careful and conducting a sophisticated balancing act between the three powers – their choice is significant and will be noted
Your report on NL is interesting – I was surprised that so many people were shy of a ‘vaccine’, I had thought only the Americans so reluctant, perhaps because they go on about anti vaxxers so much, such sloganeering does give a veneer of unique popularity
I understand your descriptions – however I had thought that like the flu this virus does pose some problem for the older age groups, even if un obese un cardiac and so on – but these too seem reluctant, I had supposed if any might be disposed to take it it would be the old
Are there any racialist discussions, minorities at risk, as per USA ? I had thought such language had infected the EU : Is the gvmt ‘advising’ ?
A table would be great, a score card, I bet Pharma are keeping many, I’ll rootle around see if I can come up with one, prices/incentives (World B, IMF, UN, China B&R) would be a bonus, could even be weighted like the Economist Big Mac index
@Gerrard White
I wouldn’t say that EU citizens are afraid of vaccines. But I would say that they’re cautions about anything that’s rushed. And many of them will realize that it may be worth the wait for a later LAV vaccine as opposed to rushing to take the early mRNA, KV and vector vaccines: put another way — why settle for fried cod now when you can have braised salmon later? Particularly when one of the varieties of cod (mRNA) has never before been tested on humans.
In reply to your query: there’s absolutely zero discussion of race with regard to vaccination in the EU.
As regards the niche group most susceptible to dying from this virus, in the EU that’s very old people with multiple underlying conditions. Most of them are in care homes, and have advanced senile dementia. Who gives permission to vaccinate such people? Many of them have DNR lockets — so is there any legal ground on which they can be vaccinated? Most of these people landed in this state before the legalization of Euthanasia in NL; nowadays, many people have life testaments that would preclude them from ever landing in such a situation.
Each nation will be able to make the decisions that are best for them. It’s notable that all are considering vaccines in some form, That puts the lie to the case that vaccines are not effective or that the uptake rate will be low.
It’s not a matter of competing between vaccines, it’s a matter of providing for the population. As long as all vaccines are found to be effective and safe, their relative merits can be compared to make the best choice.
It all comes down to the dissemination of truthful information. Good decisions will be made if that is the focus of evaluation.
The number of nations involved, makes that more likely, as it’s hard to mount a disinformation campaign within so many different cultures. Nations will learn from each other’s experiences. It’s good also that there will be many vaccine options.
@Bryce
Thank you again for your explanations
It appears that what is touted as the solution by the ‘experts’ the ‘science’ and the authorities, is not reasonably taken to be such by most of the people – across US and EU – at least not this panick rushed & dodgy technology impossible to transport mrna vaccine
How inconvenient for corporate compliance
I understand the Asians to have more confidence in the vaccines which will be presented them, as they have had in the other measures taken
The merit of the technologies, and of the vaccines, will be determined by the trials and the science. Not by speculation or disinformation or illusory truths.
Thus far the outcomes of all the vaccine trials have held promise. At least in the west, the trials will complete and will be evaluated before approval. The evaluation may be less rigorous prior to approval elsewhere, but in time that data too will be fully evaluated.
The results and the process will be made public, and if truthfully presented, people will be able to make good decisions.
On the subject of CoViD immunity:
Previous exposure to common cold infections caused by coronaviruses (30% of common colds) can provide protection against severe CoViD infection:
https://www.lji.org/news-events/news/post/exposure-to-common-cold-coronaviruses-can-teach-the-immune-system-to-recognize-sars-cov-2/
An example of: “whatever doesn’t kill you, only makes you stronger”.
Also, an interesting comment on why vaccines that are only based on a spike protein (such as the Pfizer vaccine) provide a less satisfactory T-cell response than either actual infection or vaccines using inactivated/live SARS-CoV-2 viruses, such as the Sinovac vaccine (if it works):
“Looking closer, the researchers found that while some cross-reactive T cells targeted the SARS-CoV-2’s spike protein, the region of the virus that recognizes and binds to human cells, pre-existing immune memory was also directed to other SARS-CoV-2 proteins. This finding is relevant, Sette explains, since most vaccine candidates target mostly the spike protein. These findings suggest the hypothesis that inclusion of additional SARS-CoV-2 targets might enhance the potential to take advantage of this cross reactivity and could further enhance vaccine potency.”
No, the result is saying that T-cells produced by the COVID vaccine are effective. And since previous coronavirus infection T-cells are also still present, and are known to have limited effectiveness against COVID, targeting their production as well could enhance the overall potency of the vaccine.
We know that doesn’t work against the common coronavirus because there are too many forms. But it might help against COVID.
There is no comparison of mRNA vaccine to a viral-load vaccine intended, implied or included within these results.
Thankyou for recognizing what I have been cautioning about in general.
Essential to understanding is “…that appears to be 90% effective in trials…”.
There are many vaccine development projects, some with promise supposedly. But finishing trials – sometimes with necessity of tweaking the product, then getting FDA approval, then manufacturing and distribution to cover all of the populations, will take a long time.
Meanwhile the people’s stare of BC cannot get vaccine against the perennial killer INFLUENZA in quantity in timely fashion. Yet shallow xenophobes like Hypocrite Horgan and ‘jefe’ Trudeau bash the terrible society next door that has vaccine five weeks or more earlier.
Aviation people should be challenging the narrow path of most politicians which just prolongs the virus problem. I provide advice and ammunition in http://www.moralindividualism.com/coviodgov.htm, noting the huge collateral damage in http://www.moralindividualism.com/covextra.doc.
There’s a failure to integrate, which a character points to in https://wattsupwiththat.com/2018/12/15/the-social-benefit-of-carbon/ for a different debate.
Much of this work has already been done. Manufacturing and distribution are well advanced. The trials need to continue to completion to ensure the vaccine is safe and effective. A few are expected to conclude this month, and more in the next few months. That data will need to be publicly and carefully reviewed.
EUA may be granted earlier than full approval for select groups, if the trial data warrant it. It’s too soon to tell right now, but the data we have are promising. There is more evidence for optimism, than for doubt or mistrust.
Indonesia has announced that it’s seeking to start mass vaccination in the coming weeks, starting with the (killed virus) vaccines made by Sinovac / Sinopharm in China:
https://www.reuters.com/article/health-coronavirus-indonesia-president-e-idUSKBN27T11A
From Reuters:
Indonesia has sought emergency authorisation to start a mass vaccination campaign by the end of the year to combat the coronavirus in the archipelago, the Southeast Asian nation’s president said on Friday.
“We expect to start the vaccination process by the end of this year following a series of tests by BPOM,”
BioNTech expects to deliver *300 million doses* to Europe and the U.S. in the first half of 2021.
That chimes with what’s stated above in the article, and with what we know about the impossibilities of distributing this vaccine far from its production points…which essentially restricts its use to the regions in which it’s produced.
Production is divided between sites in the US and EU. 1.3 billion doses in 2021 = 650 million doses in H1 2021 = 325 million doses each for the US and EU.
@Bryce
I found no useful tables of vaccine sales, perhaps this is still too contentious an issue
Yet more and more negative comment on the expensive and untried and impossible to transport Pfizer vaccine
Here is an article which seeks to describe one of the ways ‘science’, and ‘science reporting/publishing’, is a commodity like any other, and contains close to MSM or social media levels of concern for entertainment value overriding objective reality content
It would be surprising if it were otherwise – because that’s the very reason they tell you ‘follow the science’, take your daily dose
https://www.theamericanconservative.com/articles/the-crisis-wrecking-modern-science/
@Gerrard White
Excellent article.
I saw this type of behavior when I was at university, and later was a researcher at a prestigious research facility. Everything revolves around funding: securing funding, maintaining funding, pandering to funders…you name it. Then comes the backstabbing: the public sees researchers as selfless, devoted, pure, quasi-angelic figures that zealously work for the common good, but the reality is a wasp’s nest of opposed groups with entrenched views and personal agendas, with a huge dose of vanity and megalomania. I’ve had several papers published in prestigious journals — after which the editors see you as a potential cash cow and start to pander to your assumed ego by offering you review board memberships and invited speakerships and chairmanships. It’s an absolutely sickening circus. When I got out and switched to commercial R&D, things improved vastly, with focus on product development rather than image development; your reward was your salary increase instead of a pedestal for your ego.
Luckily, the scientific community now has the Ar(chi)ve environment on which research results can be uploaded while awaiting publication in a peer-reviewed journal: as a reader, you still have to apply a filter to separate corn from chaff, but at least you’re no longer at the mercy of reviewers and editors with personal agendas and bruised egos.
Of course, when it comes to Big Pharma, it’s an industry with an infamous reputation for buying off doctors and other practitioners to promote its products. No wonder people are cautious about vaccines.
@Bryce
I guess it should not come as a surprise that ‘science’ is the commodity over which it is the very easiest for the ruling class to operate consent and compliance control, given that they stand to make such a profit from exploiting whatever they consider useful, and given our low level of education
And correspondingly use the MSM to impose and publicise their chosen interests, in the ways you describe
The ‘follow the science’ crowd has come to play a larger role in this crisis than before, corporate compliance memes exercised via the MSM, the nerds and their acolytes is correspondingly more prominent to propogandise and to enforce the types of administrative and public health measures they can make money from
Big Pharma always used to buy off the doctors to push their products – it is ironic that there seems to be such a rejection of their vaccines in what otherwise should have been a perfect profit centre
Just some brief corrections here:
1. The mRNA vaccine distributions are far from impossible, as documented in earlier posts. Just a matter of understanding the requirements and managing them. People around the world are just as able to do this as we are. And other vaccine types will likely become available, for those who feel they can’t.
2. The science and nerds who are lambasted in these comments, are also the ones to whom we owe vaccines in general, and the incredible progress of the COVID vaccine. Ironic that even the critics here, post links from those same nerds to reinforce their views.
3. I worked in academia for half my career, have not found the conditions that are reported here. Never had a paper rejected from peer-reviewed journals, nor did I reject papers of others when reviewing. At most, there were requests for additional supporting data or explanations or clarity. But given the anti-establishment comments posted here, I can well believe those views were formed out of general hostility toward others.
@Bryce: I am not as optimistic. My understanding is 300 million doses is the *total* for Europe and U.S. Production/distribution ramp up would continue well into first half of 2021.
Taking into account of early hiccups here and there, the first 75m or so in U.S./Europe would be immensed by August 2021.
*immunized*
@ Pedro
Oh, you could be right. I was assuming that the production ramp-up was a done deal, but the distribution ramp-up will, of course, be challenging (to put it mildly).
If a more distributable vaccine arrives at short notice (such as the Moderna candidate), it may well supplant the Pfizer one.
Once the Pfizer distribution actually starts (to the extent that it gets a green light at all), it will be interesting to see what distrubution mishaps occur…assuming they aren’t covered up. I read yesterday that countries in Europe are buying ultracold freezers en masse…it seems few here have faith in the dry-iced magic box.
The dry ice magic box will still be used for transport, so still effective. The freezers are for long-term central storage to buy time for distribution. Also for larger institutions that will have significant inventories on-hand.
For smaller clinics that see less than 200 people per day, the dry ice solution (plus normal refrigeration) will work well, or they can get a small Stirling-cycle cooler if they wish to sustain longer vaccine life,
@Bryce: In an interview with WSJ, Pfizer expects to ship up to roughly 7.6 million doses daily in U.S. and Europe. Does it mean capacity is being ramped up in 2021?
The estimate of the CDC and NIH is 700 million doses available in the US by mid-2021. This is available, not administered.
The administration rate will almost certainly lag behind, but still reasonable to assume that the vast majority of vulnerable populations will be immunized by fall 2021 (estimates are about 200 million people in the US by then). That will make a dent in the severity & impact of the disease.
I have no doubt that other western nations have similar plans for rapid rollout. For sure, there will be hiccups and learning along the way. The important thing will be for people to be patient and not jump all over those to claim failure. Or to claim failure before it’s even begun.
Moderna clinical trial has reached the first third waypoint and should have interim results next week. They are expected to be similar to Pfizer. Unlike Pfizer, still blinded.
Like Pfizer, their trial has been accelerated by the surge in COVID cases, and they too will have more than the statistically required number of infections to report.
More evidence of the unbridled, hysterical paranoia in China as authorities there seek to identify (and invent) weak points in the fragile, metastable wall that they’ve built around themselves to try to keep CoViD at bay:
https://edition.cnn.com/2020/11/13/health/china-frozen-food-coronavirus-intl-hnk/index.html
At this rate, it will be a long time before tourism traffic to/from China resumes.
@Bryce
Do you mean to say China is not following the science? Bad China
Still – what has caused the recent outbreaks, if not an import?
There is a major problem, they can not stop food imports, too important: presumably they trust that their vaccine will be efficient enough to allow human travel
@Gerrard White
Just saw on the evening news here that re-infections are becoming more common…typically coming about 3-4 months after prior infection. In that respect, not unlike the coronaviruses that cause the common cold. This is what you’d expect in view of the short longevity of IgG titer, and the inability of T-cells to prevent infection (they just combat infected cells, and fire-up B-cells). Maybe the Chinese have discovered that their vaccine’s protection is not what they had hoped?
So again, there is not evidence of substantial numbers of reinfection, even within the 3rd wave which is now sweeping the US.
And again, T-cell are critical to long-term immunity, providing the necessary memory function and incorporating it into the bone marrow for future antibody production needs.
Although the antibodies themselves fade with time after recovery, the CD4 T-cells remember the virus and re-stimulate antibody production, if discovered again. And the CD8 T-cells continue to be present, to recognize and destroy infected cells, and thus limit virus production, until antibody numbers rebuild.
Together, these 3 mechanisms provide lasting immunity. How long we don’t know for sure yet, but the evidence is that the above mechanism does work against COVID for at least 6 to 8 months (the limit of the data thus far). That is significantly after initial antibodies wane, which confirms the role of T-cells in establishing immunity.
@Bryce
One of the many advantages China enjoys, some of which may also be viewed as disadvantages, perhaps, is that the people have confidence in the science deployed and in the measures taken to contain this virus, as well as at a more general level
Both this, and the level of administrative and social efficiency on display in China as well as in most of Asia, has put the ‘West’ to shame
Whatever Pfizer Moderna etc etc product is being currently hyped, it seems very likely that general uptake will be low
This is not only the result of the mishandling of the current crisis, at every level, especially in the US, but the consequence of a failed healthcare system, poor general health, and a healthy distrust of Pharma and their very selective and profit driven ‘science’
This crisis reads like a textbook illustration of the Max failure writ very large : those who fail to understand this are condemned to an ever more desperate defence of corruption and failure
As you say there is a lot we do not know about this virus – first amongst the other stupidities it is the failure to realise this that has led to the disarray and death rate in the West
The “level of administrative and social efficiency on display in China” is also on display in Hong Kong, and has similar roots.
The “people have confidence in the science deployed and in the measures taken to contain this virus, as well as at a more general level” because they aren’t given a choice.
You can argue that people in the West don’t always use their choices well, and that would be valid. Among those choices are whether to speak truthfully or spread disinformation. That isn’t tolerated so much in China, there is the government line, or jail. Here, it is their fundamental right.
The problem in the West is that the messaging has not been consistent with the science, there are too many conspiracy theories and false narratives put forward. Even by our leaders at times. And most definitely on social media, which has become a major tool for those voices.
Hence the recent labeling of false and misleading information on those platforms, and hence the exodus of those groups to newer platforms without rules. Given the choice of being truthful, they flee, because their narrative will not stand up to truthful analysis.
But no matter where they go or where they post, the truth will always catch up with them. They may sustain their theories within that echo chamber, but the truth doesn’t change.
New Zealand and some Asian democracies have been examples where those voices are free to be expressed, but are not heeded and gain no traction. Australia is moving in that direction as well.
In the US, the information well was poisoned and we are dealing with the consequences now. But the possibility of improvement is always present, and the truth and science will win out over those who have unwittingly (or otherwise) fostered the virus, in the end.
On the subject of re-infection, for some patients the second infection is more severe than the first. Virologists posit that this may be an example of Antibody-Dependent Enhancement (ADE) — a phenomenon that is notably prevalent in the case of Dengue, whereby a sub-optimal antibody actually assists the second infection rather than combating it. In the case of a normal vaccine development, one would probably “follow the science” and take some time to further study this (potentially disastrous) effect before seeking vaccine approval. But seeing as the current vaccines are being rushed, such a delay will probably not be mandated. Interesting times!
To clarify, ADE has been hypothesized as a possible outcome of COVID vaccination, but as of yet, there are no signs of it. Research into that possibility thus far has found it to be unlikely:
https://academic.oup.com/jid/article/222/12/1946/5891764
“COVID-19 Vaccines: Should We Fear ADE?”
“With others, we conclude that the differences in clinical, epidemiological, and pathological features of SARS and DENV diseases suggest that iADE does not contribute to the severity of natural human coronavirus infections Because myeloid cells are not major targets of infection, vaccine-derived nonprotective coronavirus antibodies are not expected to produce iADE infections in humans.”
As was the case in New Zealand, it’s likely the source was an asymptomatic person who was not tested. That will always be a risk until a vaccine is available. There is a small risk of transmission of cold storage packaging, that can be made much smaller still with good hygiene.
The cold storage theory fits in with the general xenophobic view of the government, so easy for them to jump aboard, but over time it won’t hold up to scrutiny, and will diminish with cases around the world.
Reuters:
Mainland China reported 18 new COVID-19 cases on Nov. 13, up from eight cases a day earlier, the country’s national health authority reported on Saturday.
The National Health Commission said in a statement that all new cases were imported infections originating from overseas.
The number of new asymptomatic cases, which China does not classify as confirmed cases, fell to 10 from 15 reported a day earlier. All asymptomatic cases were imported, the commission said. […]
https://www.reuters.com/article/us-health-coronavirus-china-cases/mainland-china-reports-18-new-covid-19-cases-versus-8-a-day-earlier-idUSKBN27U02A
@ Pedro
Very doubtful that the recent outbreak of 129 cases in a remote area of northwest China — with tightly controlled access — was “imported”. The same doubt pertains to the girl that tested positive in Auckland this week.
There’s a lot we don’t know about this virus 🤔
@Bryce: From WaPo Oct 26
“Kashgar has been an important trade outpost on the Silk Road for centuries, and it continues to be a hub for trade between China and its neighbors in Central Asia and the Middle East. The city lies close to China’s borders with Pakistan, Afghanistan, Kyrgyzstan and Tajikistan.
More than 2 million tourists visited Kashgar this month during the Golden Week holiday, according to official figures.”
Tightly controlled might be a term popularized by “Western” journalists. 🙂
Hard to learn all the facts needed from on and off, limited coverage unless regard it more like a full time profession.
https://www.washingtonpost.com/world/asia_pacific/china-kashgar-xinjiang-coronavirus-outbreak/2020/10/26/6db14e6e-1748-11eb-8bda-814ca56e138b_story.html
(Sub required)
Right now, I have little doubt, for many travelers, it’s easier to go to Xinjiang China than to Australia or NZ.
@Pedro
The region in question is where the government is currently cracking down on Uighur moslims. The external borders in the whole country are closed. If it was brought there during Golden Week, then it must have come from another area within China. Also doubtful that masses of people would want to visit a desolate, heavily guarded state during Golden Week…but who knows?
Perhaps a ferret crossing the border? 😉
@Bryce: I wonder where you read that.
From Reuters: Nov 4
https://uk.reuters.com/article/uk-health-coronavirus-china-travel-idUKKBN27L09F
China has barred non-Chinese travellers from Britain, France, Belgium, the Philippines and India, imposing some of the most stringent entry curbs of any country as coronavirus cases surge around the world. […]
The suspensions were a partial reversal of an *easing on Sept. 28, when China allowed all foreigners with valid residence permits to enter.* In March, China had banned entry of foreigners in response to the epidemic.
https://www.lonelyplanet.com/articles/trailblazers-crossing-into-china
Trailblazers: crossing into China as a Lonely Planet writer in the 1980s
@ Pedro
Someone with a residence permit is not a tourist…he or she is a repatriate. There’s a trickle of such repatriates all the time, but all of them are rigorously tested and quarantined. A border that only allows returning domicile holders in (under strict conditions) is a closed border.
If you decide in the morning that this is the perfect time to visit the Great Wall, then apply for a tourist visa and see what happens. You’re in for a disappointment.
@Bryce: My understanding is foreigners with either valid visa or residence permit.
As long as you are not from one of the countries listed, you can travel there with a visa.
From Chinabriefing:
China has decided to temporarily suspend the entry of non-Chinese nationals from a series of countries, according to their Chinese embassies, including Bangladesh, Belgium, Ethiopia, France, India, Italy, Philippines, Russia, the UK, and Ukraine. Those who will not be allowed entry into China include Chinese visa and/or residence permit holders, even if they were still valid at the time of the Chinese embassies’ announcements.
The respective Chinese Embassy and Consulates will no longer issue Certified Health Declaration Forms for such travelers.
However, entry by non-Chinese nationals with visas issued after the announcement dates will not be affected by the latest travel ban.
In recent years trading posts popped up. From QZ:
[…] Nonetheless this 5.3-square-kilometer (2-square-mile) shopping zone, formally called the Khorgos International Center of Cross-Border Cooperation (ICBC), has lured entrepreneurs hoping to get rich and shoppers trying to get a bargain.
Part inside Xinjiang Uyghur Autonomous Region of China and part inside Kazakhstan, the ICBC is a neutral territory. Visas aren’t required for Kazakhs to go to the Chinese side, or Chinese to the Kazakh side. Most shoppers, however, come from Kazakhstan and nearby Central Asian countries to buy Chinese goods: Five multi-story shopping complexes housing over 2,000 shops have been built on the Chinese side. The single shopping mall on the Kazakh side is still under construction.
Shoppers typically travel long distances on tour buses to spend the day traversing the Chinese malls. The zone estimates that 4,000-5,000 Kazakhs visit the shopping area on a weekend day. A fur-coat store owner estimated to Quartz that on a good day, there’d be around 7,000-8,000 customers.
https://qz.com/1720196/who-visits-khorgos-the-trade-zone-on-china-kazakhstan-border/(Sub required)
The Auckland case has been tracked to contact with a Military person caring for Isolation. He was asymptomatic when he passed it on. This has been the cause of 3 or 4 cases now. Genomic testing is brilliant!
And where did the military person get it?
Thanks Harry. It’s important to put the truth forward in the face of the propaganda. The source is almost always found to be an undetected but infected person.
Lots of good discussion here. Almost too much to take in, or uptake as some would say ;-). So please excuse me if my questions/comments may have already been discussed. If virus like the common cold do not impart permanent immunity once you survive it, wouldn’t the number of virus we could get eventually be so large that they would pile up in our ecosystem and we as individuals would always be infected with and battling one or more of them all the time? That fact that we are not always infected with and battling some virus indicates to me that permanent immunity would be common. Similar to the way I can understand that Bernoulli’s principle applies to the air molecules flowing along the upper surface of a aircraft wing or else they would be pilling up at some point on the surface of the wing.
Yes, this is a good point. The truth is that there is a constant process of evolution. Viruses evolve and find new reservoirs, the hosts then also evolve defenses that deny the reservoirs. The extent of viral success also depends on the degree of transmissibility, or contagion.
Periodically, a virus evolves to use humans as reservoirs, with a high level of contagion. That may last for a period of years or so at most, until the defense develops, or we intercede with a vaccine. Then the disease recedes as the reservoirs become less available.
There are exceptions for persistent diseases (like measles) that rely on transmission by new generations that are born without immunity. Those diseases are prevalent in children as the preferred reservoir. That does not appear to be the case with COVID, for which children are among the least affected groups.
That fact provides an important window for vaccination, children can be immunized before the reservoir can be established. Perhaps at the onset of adulthood, similar to the HPV vaccine. But only if the recession of COVID is incomplete, as it has been complete for H1N1 and SARS-1.
@20224T3
There are a lot of viruses on earth, with which we have learned to live
Generally speaking, until recently, in many places overall health and living conditions were improving, rendering the human response to such increasingly robust
Recently, as seen in those countries/societies worst hit by this virus, one can say that overall health and living conditions have declined, certainly this virus has provided an index
At the same time as which, and as a result of the same conditions, the influx of newly imported viruses from animals has greatly increased
This process will not cease, it will increase : the only effective counter the human can make is to improve his health and living conditions, and take significant steps to lower virus imports
The current ‘measures’ are band aids that may or may not leave too many people dead, as compared to what these societies are used to or prepared to accept, but which will do nothing to solve the dilemma, au contraire, they will provide the illusion of action without the substance
From Reuters:
University of Washington’s Institute for Health Metrics and Evaluation projects almost *195,000 more fatalities* by March 1. The biggest monthly spike of the pandemic will come in January, when more than 65,000 people are projected to die, the institute said.
A universal mask mandate in the country would save more than 68,000 lives by March 1, it said.
Biden will ask the state Governors to do the mask mandate. May go beyond that if things don’t improve. I think there’s going to be strong federal coordination now, in delivering the message on precautions
Trump did a good job in terms of enhancing the medical supply chain, spurring vaccine research, and preparing for delivery. But not in the behavioral messaging that was needed as a first response. That will change now.
I did notice at the Trump press conference on Friday, there finally was a consistent message from all the speakers on wearing masks and using precautions, saying that there couldn’t be a full opening unless that was done.
Still resistance to a lockdown or closing at the federal level. But we are getting closer to that at the state level.
I consistently wear a mask in indoor public spaces, but don’t put too much faith in them…they’re not a silver bullet.
The Italians have been zealously and consistently wearing masks since March, but they still got hit by a severe second wave…as bad now in the south as the first wave was in the north in March.
https://epidemic-stats.com/coronavirus/italy
Do they help? Probably.
To what extent? Hard to say. Models don’t take into account how people actually wear and replace their masks, how close-fitting they are, etc. When catching droplets, any mask will be greatly effective. But when trying to stop aerosols, a much better “seal” is required.
And, as you point out below, the masks come off as soon as the front door is closed. So if one member of the family brings it in (usually a young member), then it spreads through the family unit.
Interesting detail: personnel at care homes in NL can’t wear masks. Why not? The (highly prevalent) occupants with senile dementia are terrified of the masks, can’t put them into perspective, think the personnel are demons, and throw convulsive tantrums. So, just as in March, the virus has crept into care homes here again (at least 625 at present), where it methodically plucks the low-hanging fruit around it…accounting for most of our death toll. Not unlike the USA, actually:
https://nypost.com/2020/06/27/almost-half-of-us-covid-19-deaths-are-linked-to-nursing-homes/
@Bryce
Mask wearing, in the US, has become, or always was, a question of ‘manners’, in the polite middle class sense of this word
It is one of those signifiers of virtue that some of the middle and wealthier classes like to adopt, which the poor find difficult or un necessary or superfluous
As with most aspects of social life, the Americans have politicised the mask in their own curious idpol way
Following their quarrels about this issue is a labyrinthine venture into their cluster of puritanisms, secular and social, which reminds one of all those curious protestant sects which proliferated in 16th & 17th century europe
As for the NL aged, they have the same reaction as once the readers of Hobbes’ Leviathan at the sight of the masked guardians
I wonder what will happen to public opinion now that more and more (probable) re-infections are manifesting themselves…as little as three months after the preceding infection? It doesn’t bode well for the immunity conferred by vaccines. Where that’s concerned, it will be interesting to see the “decay curve” of the Pfizer vaccine as a function of time, as soon as more data comes in (after all, a base size of just 94 cases is not very meaningful). We know now from the Pfizer data that 10% of vaccinees got infected within 2 months of their second vaccine shot…but what will that percentage be after 4,6,8 and 10 months, for example? And what will the age breakdown be? To be statistically meaningful, we’ll need tends of thousands of infections, but that level won’t be achieved in phase 3 trials any time soon. So it looks as if the data will just have to come from the population at large.
@Bryce
Is this not live testing
Pharma and gvmt is desperate for something that can be sold as a ‘solution’ no matter how feeble or imperfect
They seem, the WHO etc, to have said from the beginning, perhaps only sotto voce : this is a corona and so no immunity
Or am I wrong ?
@Gerrard White
Not only that: as we look on, the virus seems to be manifesting itself more and more as being ultimately similar to the four legacy coronaviruses that cause common colds. Its fatality curve as a function of time will probably look like an exponential decay: high at first due to all the vulnerable with poor immunity, then decreasing as more and more people build up T-cell reservoirs, then trailing down to a low level as it becomes a nuisance rather than a disease…but never going to zero.
For most (non-vulnerable) people under 40, it essentially already is at the level of a common cold.
@Bryce
You are not ‘following the science’
But you are spreading anti vaxxer pessimism when we, pharma and the nerd class, have so much money and reputation to make by safely guiding you the people through this terrible crisis and have you thank us a good long while
@ Gerrard White
I saw an interview on BBC this evening with Ugur Sahin, one of the “inventors” of the Pfizer vaccine. He said that he takes the “90%” figure released last week with a pinch of salt, and that it’s more realistic to assume that, considered over a time period of months, the vaccine will predominantly help to decrease the severity of illness, and will play a much smaller role in preventing infection from occurring.
Nice to have a realist on board, instead of the “follow the science” idealists.
So again, there is not widespread evidence of reinfection or loss of immunity from COVID, within the evidence timeframe we have available right now.
The reinfection argument is put forward in order to cast doubt on the possible value of a vaccine, but it is not valid. It’s an effort to declare failure in advance of, and in hopes of heading off, success. It’s part of the anti-vaxxer message payload.
Bryce, some major misrepresentation on your part of the Ugur Sahin interview. He did not say that it would not prevent infections, he said the exact opposite. He cautioned that the 90% number is not yet certain, but said it would have more than the 50% value required for approval.
Here is a link:
https://www.bbc.com/news/health-54949799
Here is what he said:
BioNTech’s Ugur Sahin: “I’m confident that…we could have a normal winter next year”
The impact of a new Covid vaccine will kick in significantly over summer and life should be back to normal by next winter, one of its creators has said.
Prof Ugur Sahin, BioNTech co-founder, also raised hopes the jab could halve transmission of the virus, resulting in a “dramatic reduction in cases”.
In an interview on BBC One’s Andrew Marr Show, Prof Sahin said he expected further analysis to show the vaccine would reduce transmission between people as well as stop symptoms developing in someone who has had the vaccine.
“I’m very confident that transmission between people will be reduced by such a highly effective vaccine – maybe not 90% but maybe 50% – but we should not forget that even that could result in a dramatic reduction of the pandemic spread,” he said.
@Bryce
Thanks for the link- it seems that Wall Street has started dialing back on the Pfizer product and made sure the PR is scaled down
The Pfizer is too many maybe’s, almost impossible to transport, gives monetised ‘science’ a bad name, and will not sell worldwide, when Wall Street can hope more suitable champions emerge from American Pharma
So Pfizer PR has already gone from 90% effective when the CEO sells his shares to
‘maybe not 90% but maybe 50% ‘
‘I am confident we could have a normal winter next year’ is about as positive a prediction can be while remaining meaningless and utterly conditional
Anything that may cure a headache can not be that bad
I am confident that these pharma people will shill for their money over 90% of the time, and that next winter it is normal that they will still be shilling for their money
That’s a scientific prediction, 100% backed up by pharma data
The good news is that in the UK at least anti vaccine reports are to be censored because these are
‘”exploiting people’s fears, their mistrust of institutions and governments and spreading poison and harm” according to a politician
I do not think that the people waited for this Pfizer product to develop mistrust of institutions and governments, though it is probable that the Gvmt and ‘authorities’ handling of this virus crisis has not done anything in the west to reassure the people that their governments are efficient and capable
@ Gerrard White
Have you noticed that some people aren’t able to make a distinction between preventing illness and preventing infection?
Also interesting that they don’t distinguish between a live video interview with someone and a subsequent, succinct textual summary of the interview.
Because of the former shortcoming, it seems that such people are always going to be behind the curve when it comes to understanding the role of a vaccine in the present situation.
To summarize again what Ugur Sahin said in his video interview:
This vaccine is going to predominantly be an agent to mitigate symptom development, with a certain measure of infection prevention also occurring. The former (symptom mitigation) is very pleasant for the patient and the medical infrastructue in his/her country, but it doesn’t stop spread of the virus…which is only stopped by the latter (infection prevention).
@Bryce
Most people are blinded by the desperate need to do their compliance duty and serve their corporate masters – conformity is the only value equal to servility
But it is clear that there is a swingabout in opinion amongst all significant players with regard to the Pfizer scandal
The WHO comments confirm the Sanofi and the echoes from Wall Street, coupled with a toughening, or attempted toughening of the FDA as regulatory authority in order that this not be seen as corrupt as the FAA was seen to be with BA, and for the same reason, so that the EU and Asia do not automatically nix any decision
Which has resulted in the Germans co inventors saying the vaccine might or might not work – the ground is being prepared for FDA non certification and contract cancellations
The American ruling class, that part of it which counts, Wall Street, is waking up the fact that to pay a pharma to produce a vaccine which will be hell to distribute, at the expense and the responsibility of the Federal and State authorities, to a public which has told them it will not take the vaccine, and which can not be sold nor distributed overseas, leaving the market to China Russian and heavens ! the French, is to buy into yet another laughing stock of the world disaster
To follow on from every other disaster they have already brought on themselves, the gift that keeps on giving
I do not mind, the silver lining of this crisis is the chance to see how ever more stupid and wronger minded they can get – a lot dumber than it was possible to imagine
Byrce, [Edited]
The interview with Dr. Sahin is very clear, that the Pfizer vaccine offers protection from infection, as well as possibly mediating symptoms. I’ve already given his direct quotes from that interview.
Furthermore, Moderna’s vaccine results today show a similar 90% efficacy, as expected. So the validity of the vaccines is only going to become more and more evident as time goes on, regardless of the disinformation campaign mounted against them.
Here are other interview quotes. Dr Sahin assumes the worst case scenario in this one:
“If the question is whether we can stop this pandemic with this vaccine, then my answer is: yes, because I believe that even protection only from symptomatic infections will have a dramatic effect.”
Here is his view on transmission:
“While current trials of the BioNTech/Pfizer vaccine will not formally prove that it prevents transmission of the virus, as opposed to merely stopping infected people from falling ill, the 55-year-old said the high efficacy results have led him to assume it can.”
Here is his view on immunity:
““We only have indirect clues so far [regarding the duration of immunity]. Studies of Covid-19 patients have shown that those with a strong immune response still have that response after six months. I could imagine we could be safe for at least a year.”
ND has become the 35th state to mandate mask. Hard to change Trump supporters’/others’ mind.
Where I live, masks are required and indoor dining is banned. However, cases are still increasing. It’s said in many occasions corona virus is spread at social gatherings. Thanksgiving and Christmas is coming, I’m not optimistic.
Some more information on re-infection with CoViD.
A table of confirmed cases, and then an extensive list of many suspected cases. The suspected cases can’t be confirmed unless genomic material was kept from the first infection (unlikely). Note — as stated above — the interval of about 3 months between first and second infections.
https://bnonews.com/index.php/2020/08/covid-19-reinfection-tracker/
There are now more than 10 suspected cases in NL.
With regard to Antibody Dependent Enhancement (ADE), although some people might want to put the concept into an OCD box a.s.a.p., virologists are taking the matter more seriously, as evidenced from this overview article (published just this month):
https://www.sciencedirect.com/science/article/pii/S1201971220307311
For example, the following text segment:
“From previous research on ADE in other coronaviruses, in particular SARS-CoV and MERS-CoV, it appears that the existence of ADE will elicit more severe body injury, while actually reducing the viral load at the same time. This may affect the results of vaccine therapy. The presence of this phenomenon in these two coronaviruses indicates a potential risk in the vaccine therapy for the novel coronavirus SARS-CoV-2, as it shares the same viral receptor and similar genome sequence with SARS-CoV. SARS-CoV-2 may have a similar mechanism of viral entry and thus may share similar mechanisms of ADE.”
It will be very interesting to see if this will have any bearing on the vaccine approval process, or if it will just be rushed ahead blindly.
Although reinfections are possible for any disease, the numbers found worldwide thus far (25) are in the statistical noise of the current pandemic rates. Therefore not a significant indicator of loss of immunity.
Also the study quoted compared COVID to previous infectious viruses to see if there could be a similar very mild prevalence of ADE, due to similar mechanisms. The results were that it might be possible, but there is no conclusive evidence thus far that it is occurring, or would occur from a COVID vaccine.
Another key point is that the ADE response has occurred with specific killed or weakened live virus vaccines. For that case, the body can build up an immunity to the vaccine as well as the virus. Thus those vaccines may need to be single-shot as booster shots may lose effectiveness.
However one advantage of the mRNA vaccine is that it doesn’t trigger an immune response to the vaccine itself, because the RNA payload is not visible to the immune system. Therefore enhancing booster shots are possible and an ADE response is unlikely.
Again, really important to represent information truthfully and not in the context of the anti-vaxxer agenda.
It appears that Elon Musk probably has mild/moderate CoViD.
Luckily, his case is highlighting the *appalling* unreliability of CoViD testing…even the “gold standard” PCR tests, which are 20% false negative at best (and 67% at worst, if performed too soon after onset of infection).
Maybe he’ll be prompted to try to develop something a little bit more reliable? A lab in NL recently developed a rapid test that was “only” 15% false negative.
https://www.reuters.com/article/us-health-coronavirus-musk/elon-musk-says-most-likely-has-a-moderate-case-of-covid-19-idUSKBN27V017?il=0
With such unreliable testing, one can ask oneself what the point is in blanket testing whole populations, as Austria is currently planning. Sure, you might pick up some previously unnoticed cases, but you’ll also overlook large numbers of cases.
@Bryce
Thanks for this report
It is typical of the panick and subsequent cover up in the US that it takes a celebrity as well known as Musk to awaken attention to the degrees of unreliability of the various tests, which although well enough known have been disguised or rather shouted down by the ‘follow the science’ crowd as if a blasphemy
Well, if there was widespread awareness of just how unreliable the testing is, then people would start to ask how it’s possible to make meaningful policy based on bad data, and then the cat would be out of the “follow the science” bag.
I’m glad this had attracted Musk’s attention. I hope he lambasts the present testing strategy and infrastructure…time to blow some dust off the nerds.
Musk is a well-known disbeliever, has made statements questioning the reality of the pandemic since March. He is also a member of the “cure is worse than the disease” set.
Some scientists have noted that the question is whether or not he has COVID, so the correct response is to find out, not question the testing on social media. But typical of Musk who has gotten himself into trouble on Twitter before.
In this case he needed a clearance to participate in the ISS launch, and was upset that he could not.
For the record, the antigen test he took is 85% accurate for positivity, but the accuracy decreases as the person exits the viral shedding phase of the illness. So this result could well mean he has had COVID for a week or two, but happened to be tested because of the launch.
@Bryce
It was not you, it was someone else posting here who informed as to the corrupt practices of American Pharma
This widespread corruption has given rise to massive extensive and general distrust among the American peoples for all pharma peddling and products
So much so that they want no more- Notably this so called ‘vaccine’ being pushed by Pfizer at this moment
Here is a report which details a Federal Fightback, long overdue – first Insys & Purdue, criminal opoid pushers, then Novartis, now….Pfizer? who knows……they’ve drawn unwelcome attention by their corrupt pump and dump operation with this vaccine
https://www.statnews.com/pharmalot/2020/11/16/hhs-speakers-kickbacks-insys-purdue-novartis/
@Gerrard White
What a gem! Entirely consistent with what I posted above with regard to the conflicts of interest, back-scratching and nepotism endemic in the world of scientific research.
We put a lid on this in NL a long time ago. Patients who are claiming medication from their medical insurance will only be given a generic medication by a pharmacy, regardless of any particular brand stipulated by a medical practitioner in a prescription. If a patient absolutely has to have a particular brand — e.g. due to an adverse reaction to an assistant ingredient in another brand — then the medical practitioner has to justify this to the pharmacy.
It will be interesting to see what happens when multiple vaccines are concurrently available…who will push what, and how.
Important to point out this case has nothing to do with vaccine development. Vaccines are being purchased by governments for broad & free distribution, not pushed by doctors writing prescriptions. Vaccines are not elective drugs.
More news on the inaccuracy of “gold standard” PCR testing: this has been known since the summer, thanks to research from Johns Hopkins. The “false negative” curve in the middle of the article is astounding.
https://www.abc.net.au/news/2020-07-15/covid-19-testing-not-as-accurate-missing-coronavirus-cases-grow/12455076
So Elon Musk is just the latest to point out the unreliability of the present testing regime. Every country now has personalities with similar experiences: just 2 weeks ago there was a prominent mayor here in NL who needed two tests a few days apart to confirm that he had CoViD, even though the pathology made that abundantly clear from day 1.
But it’s more convenient for OCD boxers to just dispel this as “illusory truths spread by an anti-vaxxer”.
@Bryce
When criticism of Pharma dubious and illegal practices come from one section of the ruling class, the other section has to blame the commies
Such internecine feuding is bad for business, so when Wall Street decides who and what will distribute the vaccine, they all shut up and say yes sir
Is’nt Elon the same guy who’s wiping the floor with Boeing on the into Space adventure?
Yes, it absolutely is illusory truth, and the inclusion of testing accuracy is part of the list-building required to support it.
Any exception, though massively in the minority o cases, then can be pointed to as supporting the illusory truth. That is part of the methodology of disinformation.
For the record, the PCR test is 95% accurate for positivity. The fact that it’s not 100% does not mean it has no value, or can’t be trusted. Pure disinformation.
@Gerrard White
Not only are there people who don’t understand the difference between infection prevention and illness prevention (symptom mitigation) when it comes to a vaccine, it seems there are also people who don’t grasp the difference between false positive and false negative when it comes to testing. Can you imagine that?!
To clarify for those who don’t have much acumen:
– False positive only has an economic downside, because the person concerned is unnecessarily staying sequestered from his surroundings, and thus can’t work.
– False negative has a serious epidemiological downside, because the person concerned can move through his environment and spread illness, under the illusion that he’s not infected.
With this type of ignorance around, no wonder the whole testing/isolation strategy is a shambles.
AP: Surging virus cases get a shrug in many Midwestern towns
https://apnews.com/article/iowa-south-dakota-coronavirus-pandemic-nebraska-north-dakota-bf7197b284401dea8b779cfa764dfab2
‘ Jenna Lovaas, public health director of Jones County, Iowa, said even now that her rural county has the state’s highest virus rate, people have opted not to make any changes, such as protecting themselves and others by wearing masks.
“They don’t think it’s real,” she said. “They don’t think it’s going to be that bad or they just don’t want to wear a mask because we’ve made it a whole political thing at this point.”
‘ Although doctors and public health officials have criticized the governors for their lack of action, voters in all of the states last week backed Republicans, including President Donald Trump, who has mocked mask wearing and downplayed the seriousness of a pandemic that has killed more than 240,000 people.
That has left Midwest medical professionals wondering how they will reverse a tide of people being treated for the coronavirus if residents of their states still aren’t taking the illness seriously.
Poor Iowa.
15% over 65 (much the same as Europe) but 30% obese (twice the rate in Europe), and not that many large urban centers with sophisticated hospitals…ouch.
There is a common misconception that “big, strong men” will just brush off CoViD…but, in reality, obese men are statistically headed straight for the ICU.
@Bryce
As per the post by Pedro on Iowa, it looks like the people distrust their gvmt and authorities more than they fear the virus
With good reason
Distrust and disbelief in the gvmt has been building for a very long time for very good reason, the bug is brand new
As you report from the NL even the most susceptible portions of the people declare their reluctance to take the first vaccine – this is not because the people are stupid, it is because they are intelligent
The ruling class and their acolytes is always perplexed when the people disagree and disobey, they then blame commie outsiders and foreign agents, and dial up on propaganda
@Bryce
From AFP interview with Kate O’Brien, WHO
Immunisation Chief
https://asiatimes.com/2020/11/trust-in-vaccines-vital-to-beat-pandemic-who/
http://www.jamaicaobserver.com/your-health-your-wealth/trust-in-vaccines-vital-to-halting-pandemic-who_207757?profile=1754
« More needed to be done to boost public “confidence in the fact that the vaccines that WHO is involved in evaluating, we will not be compromising on safety or efficacy”, she said.
O’Brien acknowledged that there were a number of outstanding questions about the Pfizer-BioNTech vaccine candidate and its peers, including how long protection against the virus would last.
And while the vaccine candidates are being tested for how effectively and safely they protect people from developing the disease, it remains unclear whether they actually avert asymptomatic infection and transmission of the virus.
A big question, she said, is: “does it change your likelihood of transmitting to anybody else?”
“The goal here is that every country should be able to immunise 20 per cent of their population by the end of 2021,” O’Brien said.
Meanwhile, the logistical challenges of getting approved vaccines out to billions who need it are daunting, from manufacturing to ensuring the transportation and storage at the extremely low temperatures some of the candidates require.
“A vaccine that is highly efficacious and is safe… still is only valuable for a public health impact if it actually gets to the people that it needs to protect and is used widely in populations,” O’Brien said.
Developing a safe and effective vaccine “is like establishing base camp at Everest”, she said.
“But actually getting to the impact of vaccines is [like] having to climb Everest.” »
?20% world pop immunised = ‘back to normal’?
That’s the bad news – here’s the good news-
More pushback against Pfizer – this discrediting of Pfizer from experts authorities and Wall Street seems to growing stronger – first Wall Street, then WHO, now : here’s Sanofi
https://asiatimes.com/2020/11/sanofi-says-its-vaccine-wont-need-supercooling/
Who said commercial competition was a bad practice ?
There is no pushback against Pfizer in this article, or in the others. It acknowledges the cold chain problem that has been addressed. Any new vaccine that is effective and safe will be welcomed. As has been said many times, no one manufacturer can supply enough, quickly enough, for the world.
The concern about transmission rates applies if the vaccine only lessons severity of the infection, as an asymptomatic person still can transmit the virus. However it appears from the preliminary data that the Pfizer vaccine does prevent infection, therefore will reduce transmission rates.
The developer also says it lessens severity for those who do become infected. That was not released in the preliminary data. So we will know more when the data are released.
@Gerrard White
Thanks for these links. Of course, Moderna had already advertised last week that its vaccine doesn’t need to be super-cooled, and the Russians jumped in to tout a high (and unlikely) efficacy of their Sputnik V vaccine. All part of the pre-release posturing and PR. The kitchen is starting to get crowded with a lot of increasingly vociferous cooks. And then authorities have to wade through that mess and try to create a distribution scheme? That’s a challenge!
But you should remember that Aspergers have difficulty reading between the lines and can’t pick up on subtleties , so the message will not be universally grasped.
@Bryce
This looks like a normal jockeying for position amongst various trade groups and regulatory authorities
The EU and the RECP are both much more significant in terms of population and influence than the US – what took Wall Street and the FAA some time to understand has now taken much less
There are still a few exceptionalists and isolationists in America, but their servility is only equaled by their stupidity
Wall Street has moved on – in fact the natives are more useful to them in their current state
@Bryce
This link reveals a world, well that tiny part taken up by the UK, deeply divided against itself – indeed in chaos
https://www.dailymail.co.uk/news/article-8952939/NHS-workers-join-anti-vaxxer-group-compares-Pfizer-jab-poison-opposed-masks.html
“NHS Workers for Choice, No Restrictions for Declining a Vaccine surged in size
The group compares the Pfizer jab to ‘poison’ and is opposed to wearing masks
Members include GP worker, A&E nurses, healthcare assistants and lab workers
Health Secretary Matt Hancock branded the group ‘entirely inappropriate’ today
Four out of five want people who spread fake vaccine news to face prosecution”
The good news is that it looks like there’s a new pump and dump Vaccine coming through
And the disinformation campaign invents things between the lines to avoid the direct truths. Extremely clear evidence of that in these posts.
But the truth ultimately can’t be avoided for long. More good news about vaccine development today. That’s likely to continue as we move forward.
You exaggerate and confuse.
‘Big’ is vague, some people are big but fit. (FAA had to be taught that re neck size screening for OSA. Some athletes are – the star of my high school basketball team was like a thick plank, muscled of course. Exercise like lifting weights probably makes neck large.) Tall seems big if shoulders are in proportion.
‘Obese’ is being used too vaguely these days, threshold too low thus efforts spread too thin.
The risk for COVID-19 is specific to the equivalent of swelling for other reasons, not good in the face of COVID-19.
Obese correlates (which is not causation) with diabetes which if not controlled damages organs thus ability to resist, AND with bad diet. Lack of exercise.
I say ‘Sit on a couch eating pastries all the time and you will become a deteriorating potato.”
Voilà.
Lots and lots of studies on this subject…this is just an example. The problem with obesity in the US is that, because it’s so prevalent, people are less likely to recognize it as being a sub-optimal corporeal condition.
https://www.sciencemag.org/news/2020/09/why-covid-19-more-deadly-people-obesity-even-if-theyre-young
And if causes of obesity affects the individual’s heart that adds to risk from SARS-CoV-2 because COVID-2 is probably in significant part a vascular disease not just a respiratory disease.
Stackup of risk factors is what does one in, a major proportion of deaths from infection with SARS-CoV-2 are of persons who have several serious health problems, besides lungs and cardiovascular system there are kidney and livers.
Yes, this is the product of the misinformation campaign that is conducted here and elsewhere. Those people have been told those measures don’t work and that the cure is worse than the disease, so they choose the disease. We see the same thing in my neighboring state.
The only solution is education, to undo the propaganda and get the correct message out there. Examples like New Zealand are important to that message, that’s why they are attacked (notably with the same cure is worse than the disease argument).
The vaccines should come online with a new administration. Then there will need to be a similar educational campaign to undo the anti-vaxxer message.
It helps to remember there is still a majority who do follow the guidelines and are receptive to the correct messaging. The example they set, along with successful results, will eventually penetrate the other resistant groups.
https://mobile.twitter.com/VOBOE/status/1327951846674231298
https://mobile.twitter.com/JodiDoering/status/1327771329555292162
The FiveThirtyEight website has done a great analysis of disinformation methodology, in terms of the US election results and how they were perceived by Trump supporters But the method also applies to any disinformation campaign, such as for COVID protective measures or vaccines.
The basic sequence is this:
1. Priming — the speaker claims/predicts failure or bad outcome of an impending event based on false or misleading information, well in advance of the actual event. This sets the stage for the illusory truth.
2. Illusory truth — the speaker sets up an illusory truth that is the payload of the campaign, by casting doubt and distrust in the legitimacy of the truthful outcome. This is done by an extensive list of false reasons why the truth should be doubted or distrusted, and sets up the illusory truth as being supported by those false reasons.
3. Confirmation bias — by being provided with false reasons that support the illusory truth, the audience is primed to look for evidence of those reasons in isolation, and then use them as confirmation of the illusory truth.
A lot can be learned from this analysis. In the election, the priming was that the election would be stolen by fraud conducted through mail-in ballots. The illusory truth was that this was a common outcome, and was responsible for Trump losing the popular vote in 2016. The list of reasons given were ballots being destroyed or not counted, dead people voting, people voting multiple times, widespread cheating, etc. The payload was to cast doubt on the legitimacy of mail-in ballots and their impact on the election. This was further engineered by encouraging supporters to vote in person.
Then on election night, the in-person ballots were counted first, creating a red-shift and giving Republicans early leads. But as the mail-in ballots were counted, the red-shift was corrected and the Democrats took some leads, including from Trump.
In the minds of those who had been primed, this was confirmation of the illusory truth, which was that mail-in ballots would steal the election. The evidence was right there in front of them, Trump won but the mail-in ballots took the victory from him.
In retrospect, society didn’t do enough to shoot down or counter the initial claims of the priming and illusory truth. Mainly because they seemed fairly far-fetched, and had no supporting evidence. But now the true impact is revealed, it didn’t matter whether those claims were true, once they were established. Those people (including Trump) now believe the election was stolen from them.
So the lesson is, don’t let the falsehoods get started, answer with truth early and often. Interrupting the sequence is a critical step to prevent the illusory truth from becoming established. Consistent messaging is also key. In the case of the election, the messenger-in-chief was an unreliable narrator.
The scary part of vaccine development is that gummint types aren’t always clear responsible thinkers. While The Donald has been criticized for flapping around, Biden and Harris are even more use emotions as their means of knowledge (inherent in their underlying ideology).
And medical people don’t always do well. The main hospital in Nanaimo BC went six months using the wrong strength of bleach solution (sodium hypochlorite) to wash walls, while struggling with one of the common infections. Sounded like they were using something closer to what is used to make water drinkable, rather than the ‘shock treatment’ concentration used to disinfect a water system (then flushed). Plenty of information readily available in the region, someone did not check or did not listen to staff.
More on PM and paying attention:
CPAir and Pacific Western believed in preventative maintenance. It was key to PW’s 707 operation (with one airplane some years), various contributors but also shoulder seasons giving time to fuss over things.
Pacific Western and Wardair filled the FE seat of 707s with experienced mechanics trained for the seat, they kept a close eye on the machinery and communicated with maintenance people. PW even had a dedicated crew that met the airplane at the terminal to get immediate information, ask questions, and attend to needed work. They’d come in from home if needed to meet the airplane if it was way off schedule.
Then a jerk maintenance director eliminated that crew. He also forbid mechanics talking to pilots about problems with 767s in early service, fortunately they often ended up at the same table in the employee cafeteria in the bowels of the terminal, where they diagnosed a pattern to one recurring problem and devised a solution. (Problem was airplane systems got confused if power was cycled at some point in maintenance such as up on jacks, their solution was to have mechanics taxi the airplane from hanger to terminal and cycle flight controls enroute. PW had mechanics authorized to taxi airplanes.)
Pratt and Whitney once did a study comparing what I term run-to-fail with PM, finding little difference in cost because of the high cost of airplane out of service, especially if stuck somewhere. (I exaggerate, there are inspection and overhaul periods, but PM included a higher standard of condition out of the overhaul shop.)
Vaccines of course need excellent quality control.
Supply of vaccine against the perennial killer INFLUENZA has many times been further delayed in Canada because one of the few blessed suppliers had to throw out a large batch.
That’s a message for politicians looking for a quick fix.
(Leeham economic advisers might note the pathetic, almost laughable, fiascos with production of cannabis in Canada.
Huge batches thrown out, in one case the original plant was OK but there was little QC in the expansion next door.
Red ink in the streets, not just blood from intoxicated drivers like the out-of-control ones who continue to maim people in the Victoria BC area. Many startups failed, some bought out by others who I wouldn’t invest in even if I would stoop to helping produce intoxicants.
Accidents include an out-of-control bleep who ran over a lady on her scooter, she may never function well again. Earlier an idiot who maimed a person in a crosswalk while turning left one foggy morning – taking medicine for pain from an eye operation he had, plus marijuana for pain.
(Do doctors have to call police to check on their customer after the operation and early the next morning?)
Yet politicians whose beliefs are founded in Marxism act against policing.
PFIZER AND BIONTECH CONCLUDE PHASE 3 STUDY OF COVID-19 VACCINE CANDIDATE, MEETING ALL PRIMARY EFFICACY ENDPOINTS
“Primary efficacy analysis demonstrates BNT162b2 to be 95% effective against COVID-19 beginning 28 days after the first dose; 170 confirmed cases of COVID-19 were evaluated, with 162 observed in the placebo group versus 8 in the vaccine group.”
https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine
PFIZER AND BIONTECH CONCLUDE PHASE 3 STUDY OF COVID-19 VACCINE CANDIDATE, MEETING ALL PRIMARY EFFICACY ENDPOINTS
“Efficacy was consistent across age, gender, race and ethnicity demographics; observed efficacy in adults over 65 years of age was over 94%.”
https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine
PFIZER AND BIONTECH CONCLUDE PHASE 3 STUDY OF COVID-19 VACCINE CANDIDATE, MEETING ALL PRIMARY EFFICACY ENDPOINTS
“Data demonstrate vaccine was well tolerated across all populations with over 43,000 participants enrolled; no serious safety concerns observed; the only Grade 3 adverse event greater than 2% in frequency was fatigue at 3.8% and headache at 2.0%.
Companies plan to submit within days to the FDA for EUA and share data with other regulatory agencies around the globe.
The companies expect to produce globally up to 50 million vaccine doses in 2020 and up to 1.3 billion doses by the end of 2021.
Pfizer is confident in its vast experience, expertise and existing cold-chain infrastructure to distribute the vaccine around the world.”
https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-conclude-phase-3-study-covid-19-vaccine