Leeham News and Analysis
There's more to real news than a news release.



Bjorn’s Corner: Do I get COVID in airline cabins? Part 2.
May 15, 2020, ©. Leeham News: In our Corner series about flying during the COVID-19 pandemic, we dig deeper into the knowledge around when a person is infectious and what to do about it in a air travel setting.
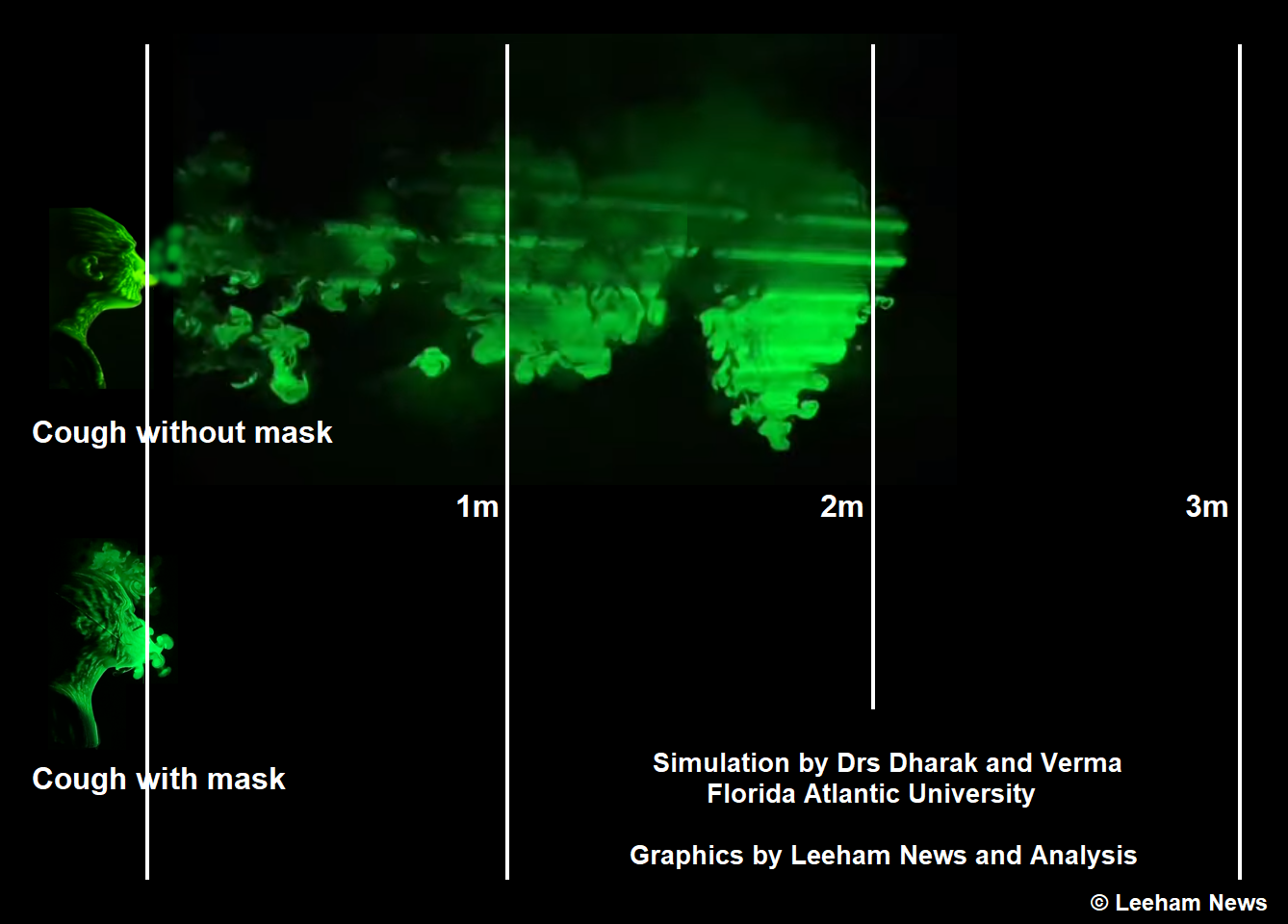
Figure 1. Droplet cloud when coughing.
What is known about COVID-19 virus transmission?
The key to getting air travel to restart is to find ways to avoid passengers infecting each other and airport/airliner personnel. This involves the whole event, from leaving the car or public transport at the airport until one enters public transportation or a car at the other end.
IATA (the airline association) has published additional information this week on top of what we referenced last week. We also got a tip of an even deeper information source. The German public broadcaster NDR has made 41 (so far) podcasts around COVID-19 with Professor Drosten, the lead virologist of Berliner Charite’, the top German research hospital.
You find the German podcasts here.
Each interview is transcripted, and all research studies Drosten comments around are referenced in the transcripts. A virus expert condenses decades of worldwide virus research and knowledge around COVID-19 for us.
The key insights that are relevant to air travel from this series:
When is someone infectious, and how to detect it?
We now know, according to Drosten, that a person that gets infected with COVID-19 is infectious two days before he gets symptoms, with his most infectious start the day before symptoms. After a week, you don’t infect other people anymore.
But, detailed research, with repeated 100% testing over time in an isolated village in North Italy, shows 44% of infected persons are symptom-free! They have no knowledge they are infectious or have COVID-19.
This explains why IATA, in COVID-19 information issued earlier in the week, says checking the temperature of passengers before they, for instance, pass security has limited value. It might still be done, but more for reassuring passengers than effectively stopping infectious passengers to board planes.
The adequate checks are so-called PCR swab checks that detect the existence of COVID-19 viruses in a person’s nose/mouth. Right now, PCR checks that are practical to use around the check-in at an airport are a few months away.
My comment: When they are with us, they should form the base for a re-established air travel system without the need for further checks and quarantines.
Do masks help?
Given that you don’t know if you (or any other person) are infectious, does everyone wearing a mask help? Yes, it does, says Drosten.
A detailed study in Hong Kong found no trace of viruses in the exhaled air from virus-infected persons wearing standard cotton masks.
At the same time, persons without masks had viruses in their exhaled air (the study sucked up all exhaled air during 30 minutes from persons infected with different types of viruses, including Coronaviruses).
Drosten emphasized masks stop you from spreading viruses to others; it’s their most crucial function. Even simple masks diffuse the exhaled air jet, Figure 1. Their stopping of a droplet jet means wearing any mask type is better than none.
My comment: As half of us with infections don’t know we’ve got it, we protect others by wearing masks. Wearing a mask is comforting, as this reduces the risk of me infecting others.
The protection of airport and airline personnel
IATA gave further information about the risk to persons working at the airport and in the aircraft.
The airport and airline personnel that are interacting face to face with hundreds of travelers each day need the best possible protection for their nose, mouth, and eyes. Here masks and eye protection to hospital standards are motivated.
The relative safety of the traveling passenger and the risk to the crew we talked about last week is supported by further statistics that IATA provided.
We dig into this data and other studies around the risk of passenger-to-passenger infections next week.
The name of the German virologist is Drosten not Drosden.
About 50% of the people with a COVID-19 infection will develop no symptoms, e.g. no fever. According to many studies additional 12-25 of the people with a COVID-19 infection will develop symptoms at a later stage, but are already infectious without symptoms. So far that means with temperature screening you would miss 62-75% of all infected people.
And then there is another effect. The WHO and other authorities know from other epidemics one thing for sure: If people are afraid to pass a temperature screening they simply take a fever suppressing pill before. Such pills are available everywhere. No need to visit a doctor and get a receipt.
Therefore WHO, European Centre for Disease Prevention and Control and many others say, that temperature screening is nearly useless. But still some airport are implementing temperature screening now…
What we really need and what would solve our travel problems is a cheap fast test. Many insitutions are working on lateral flow tests with saliva for COVID-19. Lateral flow test? That’s the principle of e.g. pregnancy tests. It was invented 40 years ago. And such pregnancy tests are today produced in China for about 1 Cent per piece. It’s just a small plastic strip with tiny amounts of some “substrates printed” on. If we would have such cheap tests, then we could test passengers before entering the airport, before entering another country and so on. Such tests are not as precise as a PCR test, which can detect the smallest amounts of the virus. But we would find all people with a high virus load.
Thanks Guido.
Fixed the typo and good info on the temp and test side. This kind of test should be good enough and we could skip temp scan which is more show than useful and the dreaded quarantine on arrival, it serves no-one.
Temperature control is useless.
https://en.wikipedia.org/wiki/Antipyretic
The figures I’ve seen suggest that thermographic fever screening may detect up to 20% of infected if both departure and arrival screening is used. Even if only 5%-10% it’s worthwhile given its lack of intrusiveness. It will also discourage some passengers from knowingly travelling sick as well as slowing the spread of other colds and influenza.
The economic problems created by this pandemic are so serious that I believe it will be necessary to require passengers to declare that they are not knowingly sick with infection when travelling, to obtain doctors clearance, and that knowingly making a false declaration is an offense. It would be hard to secure a conviction but every measure must be taken.
To reduce the contagion between passengers, it should be possible to pipe the overhead air outlet to a breath piece, like the emergency oxygen mask. No need to be airtight, the positive air pressure should be enough to avoid contamination.
Per the prior Corner on this subject, the airflow is positive top to bottom and likely will likely preclude it already.
The HEPA filter system will remove it.
If my understanding of you idea is correct, you would rather need a negative pressure in your breathing device in order to make sure the virus goes through the overhead outlet. Sadly this would preclude people from breathing…
In addition, it would require a complete modification of the air conditioning system… and each passangers breathing device should be replace after each flight…
Potentially a good idea, masks are quite difficult to breath through over longer periods and positive pressure would make it possible to wear longer periods plus we now have a system that provides Oxygen when needed and complete protection against smoke inhalation till evacuation. I think it would have to be an optional requirement and quite some sanitation will be required. I had thought that a mask type known as a CV95 could be used during boarding and takeoff until seat belts sign was off. This type of mask protects against smoke and chemicals and would provide some protection in event of takeoff crash.
If air circulation is indeed 20 cabin changes per hour it implies an average downward air flow of about 2cm/second. This is quite a lot and takes air out of head high inhalation within 20 seconds. It appears to be effective given public transports poor ventilation compared to aircraft and its higher infection rates.
My own view is that if passengers wear masks except when seated the risk has been dramatically reduced and then all we need is a way of keeping the toilet clean. The seat back rests must produce a considerable barrier to flow.
The main risk for getting Covid-19 when flying somewhere is in the taxi and at the airport terminals in lines for security and boarding. I beliave on most aircrafts air recirclation can be shut off. Then all return air from the cabin will be go overboard instead of some % going back and being mixed with fresh air from the air cycle machines. Hence aircraft cabin air is much cleaner than hthe aiport terminal air on average.
PRC? PCR!
https://en.wikipedia.org/wiki/Polymerase_chain_reaction
While Bjrons information is technically interesting and worth publishing, its not the whole picture. We tend to be parochial. Unlike a MAX issue, you can’t program the problem out, its not airplane specific.
While my survey is not real valid, the people I am in contact with will continue to limit public contact, not travel until a vaccine is in place.
Prior to lock downs the data shows the public was pulling back from travel, eating venues, sports etc in massive numbers.
Safe on the plane and not safe getting to the airport, from the airport or at your destination and whatever you are going there for is a complete package.
I don not see it is going to return even close to normal until its squelched and that means vaccine.
@TW
This is right, making all this effort for air-t while the rest of life is not cleaned up is a similar manner is pointless – imagine all this on metro systems where 100x pax air travel every day (200x?) or in factories or offices (100,000x?)
but it is, increasingly, being said that a vaccine is not coming soon, and even if it does it’s going probably to be seasonal flu type jab effective, only
so? solution: clean up health and healthcare – this going to take a generation or more
and bite the bullet – herd immunity, another seasonal disease, fewer people cardiac or obese, overall result perhaps positive, perhaps negative, but nothing like the massive health (and all the other) problems caused by mass unemployment and poverty
This is one of the arguments for herd immunity in Sweden, If you lock down the population, how do you unlock without a resurgence of the virus? Essentially you have to find a way to lock down the virus instead of the population. Air travel is just one aspect of that. I think there’s going to be an extended learning curve to figure out all of this.
@Rob
You can not lock down the bug – it’s out everywhere – all you can do is grade the fatality rate at the initial epidemic, even so this has been more than difficult
To use air travel as a paradigm is misleading – it is a tiny fraction of the environments to be controlled and the very much easiest to control by a long way
Bugs are produced by, it is generally said, the intrusion of ind ag into every corner and ever increasing massive factory farming of animals
There will be more and more bugs before the sufficient sanitary reforms of these environments are implemented and reductions in scale are made
The US is in chaos and wants to stomp the bug, that’s not an option
Pity poor Vietnam – they controlled the bug beautifully, but now what? Quarantine every traveler? Stop and scan or track and trace a major part of the population in perpetuity?
So- what to do about the sufficiently distinct mutation or the next bug on it’s way this autumn?
Build 100x more hospitals, stockpile billions of masks, onshore major parts of the medical industry?
Or ?
Gerrard, I agree. I was just pointing out the lockdown options (isolate virus or people), not saying it was something readily done.
New studies are saying the initial R0, before intervention, may have been as high as 5 or 6 in Wuhan. The effects of non-intervention also may be too high to deal with practically, so maybe a hybrid approach is needed, as William suggests.
https://wwwnc.cdc.gov/eid/article/26/7/20-0282_article
Sorry, got my maps confused here. In Sweden the daily new cases are less than 1K per day. So the calculations above are wrong.
The estimates of undetected cases per detected case in Sweden vary widely (7 to 70) so it’s difficult to say how many cases there actually are.
It’s interesting that in Sweden, the impact of not locking down has not been as great as expected (less infections than predicted). While elsewhere in the world the impact of locking down has also not ben as great as expected (more infections than predicted).
So that may mean things are more complex than we understand right now, with many factors being in play.
Sweden is doing it right. The infection rate for COVID-19 is R = 2.5 which is much higher than influenza which has R as 1.3.
When 60% of the population has had CVID-19 and is then more resistant than any vaccine the disease will stop spreading, 60% = 1-1/2.5. Nothing will change this, a lockdown only delays this while causing worse devastation and therefore has no point apart from providing some time to isolate vulnerable groups and prevent the saturation of healthcare and test some treatments.
If increased hygiene is implemented and we can cut the transmission rate to flu like levels of R = 1.25 then only 20% of people require immunity to stop the spread 20%=1-1/1.25. All this requires is mask wearing in shops and public transport and hand hygiene. How far we can go with hygiene is a question but clearly public transport needs dramatic changes in the way touch terminals, masks and hand grips are used.
Giant pop concerts can disappear, no great loss, they’ll soon be replaced.
I admit, now I’m confused. Some weeks ago they’ve modelled it would take 20 years(!) to have 60-70% of infected people overall (which means herd immunity) with spreading levels at that time in germany. The US currently have 5% of all people already infected, numbers from germany arfe roughly in the same ballpark. Source: Drosten
As for all calculations you have to assess the end result – is it realistic?
Can sweden reach 60%-70% so much faster?
That spreading differeny would be *enourmous*. Are there any numbers available at which level sweden is currently?
Sweden estimates they have an Ro now hovering about 1.o, which would imply a doubling of the infected population every 4 days. They began above 2.0 in February, decreased to around 1.5 in April.
Actual new case numbers are about 70K to 100k per day, from Johns Hopkins Coronavirus map for Sweden.
So crude math is 10M population divided by 100k per 4 days, gives you roughly 400 days, but herd immunity would be reached before that.
People can have twice or three times, challenging the herd immunity believers.
Yes, but the reinfection rate seems to be small (under 5%) and it’s not clear yet whether this is a reactivation of dormant virus in the body or a second new infection.
Some doctors have pointed out that an initial mild infection may result in a weaker immune response, so the virus looses the initial battle but can rally. This is seen as well in the common cold virus.
Doesn’t necessarily invalidate the concept of herd immunity, which we know to be correct in general, but raises questions as to how much time would be needed to achieve it.
@Rob
the choices are not limited to ‘intervention’ – by which I take you to mean lockdown, and ‘non intervention’, I suppose you mean not lockdown, although the term is euphemistic
there is the Vietnam approach – but however successful initially, it merely requires the problem be re stated in the same terms at a later date
the longer you wait, the more likely bugtwo appears, panicking about two bugs would be even more hair on fire
agree with you that lockdown is a panic response – but once panicked twice shy is not a dictum you can be sure the governments will rely on
this is a dilemma with only bad solutions or worse solutions
but clearly the very worst solution is on display in the US – this should be sufficiently apparent to install a certain amount of reflection as to why so
(bad health, worse healthcare, in ability to prepare or learn from history, immature politics, no ability to design & co ordinate overall strategies or policies, short termism, technobabble replacing realist or practical approaches, the immediate recourse to ‘war’)
Note: Sweden has locked-down nursing homes, and such senior age population goings-on.
Sweden did right and wrong. They missed out the spread of the virus to elderly homes by caretakers that was not classified as medical staff hence limited training, protective equipment and mainly porly paid immigrant workers seeing 12-20 different elderly every week spreading the virus being emplyed by private comapnies often ran by other immigrants. Hospitals and medical staff got the equipment they needed eventually and the not so dense population kept distance and limited the spread. Testing slowly picked up and are now at pretty good weakly capacity.
Had the Western world had powerful computer software simulations running the Virus DNA as soon as it was publicised in China around dec 31 they they could have concluded the severity of it and closed all borders the first week on Jan-2020 saving a few 100 000 lives.
@claes eriksson
every country got it wrong this time, previous bug outbreaks had been contained along the lines you mention
why not this time – it is the key
it is clear that once it is ‘out’ in any widespread way, it is impossible to do more than contain it for a while or better protect the ‘target’ , old and unhealthy people
as you point out the capitalist healthcare system is in efficient
it might be easier, instead of lockdown quarantine and so on, the start to solve the problem the other way round
greatly reduce if not ‘eliminate’ the numbers of unhealthy old people, for example, it is not a given that the two are inseparable, until of course the very end of life
perhaps the next bug will circulate unknown for longer and so be impossible to control by traditional track and trace detection
and cut down on the meat pits which, it seems, breed the bugs, in Asia as well of course in the rest of the world
There is something absurd about 1 million people per day crammed 50-110 people per day in a bus or carriage spreading nasal mucus as they touch hand grips in a poorly ventilated environment. The average person using 8-10 ATM machines per month (10 million Potential spreading events) and using keypads and screens at super markets, airports or petrol stations just as often. We’ve created an absurd situation that mimics the environment of a million animal bat cave. None of the technologies have been designed or regulated in regards to control of transmission of disease even though many have warned. Its likely fairly simple regulated measures such as bacteriostatic coatings, Compulsory ventilation and filtration Standards in buses and windscreen whispers on touch screens that deploy an antiseptic cleaner would go a long way. Vaccines are definitely the silly way to go.
@william
As far as I understand vaccines in general, the proliferation of antibiotics and vaccines, are short term answers which break down in the long term and leave the human herd immune systems weaker
it is said that the massive overuse of antibiotics in factory herd animals did forawhile suppress disease at the expense, if that is not ironic, of fattening the animals by a great margin
which obesity was passed on to the habitual flesh eaters, and is one of the prime sources of the overgrown obesity on display all around the ‘western’ world
in turn the bug loves the obese to death, ditto the cardiac arrest, and pretty much everything in nature picks on the fat to feed on them or to get rid of them
the ‘pill for every problem’ attitude turns out to lead to short termism for humans once a new unpillable bug comes along
what is needed is something new in human health rather than a war plan for every bug on the march
PRC swab test is the main one used in France for Covid-19 detection. Although the test by itself is pretty reliable (>95% of positive tests are effectively positive), the results are highly sensitive to the way the sample is taken and the “chance” for the virus to be at the food place at the good time. Some statistics evaluate that 40% of negative tests are in fact positive…
As an example, a friend of mine who had all covid-19 symptoms was tested 3 times and always negative.
That said, for the time being, PCR tests are still far better than other means such as temperature screening.
However, PCR tests are pretty uncomfortable when performed… I doubt any passengers will be eager to go though it for each flight…
Depends too on the physical location the sample is taken in body. It could be a inside cheek swab, or the most common one here a deep nasal swab and the 3rd one sample from deep inside the lungs.
From what I can see the nasal test may miss virus that is now inside the lungs doing its nasties, this may happen because you havent breathed it in, but hands touched the mouth.
Are you aware this depends on the stadium of his desease ?
Its only possible to identify the virus from deep throat samples in the first week after start of symptoms. Later on the virus may be present in his lungs but not nearly massed enough in his throat anymore. This fact was not widely recognised in the beginning. Many patentients in Wuhan could only be diagnosed by symtoms and CR pictures of the lung (there is a typical pattern to be seen). You could also get fluid samples from the lung, which is seldom done.
That’s also the reason for beeing infectious during the first week only.
Source: Drostens podcast.
Any globalisation of passenger test sample collection and analysis may open another subject with potential legal ramifications: PRIVACY.
We are speaking here of personal human samples recovery and manipulation; such activities are in many countries highly supervised / restricted… and authorisation are limited to healthcare organisms.
Who may do it in airports and hold the them? Private companies?
How to ensure these highly personal data are not used for other non declared purposes? That other analysis are not done? How to ensure anonymity and privacy?
Testing people before flying is a good idea for sure but side-effects have to be carefully looked at.
Otherwise, GAFA practices revealed by Cambridge Analitycs affair may soon appear pretty little player by comparison
What Privacy? All my financial information as well as my security clearance info when I held it have been compromised about 10x over.
Every hostile government and criminal in the world has all my info but me!
From Boeing:
https://www.flightglobal.com/airframers/boeing-to-model-potential-spread-of-pathogens-inside-aircraft-cabins/138402.article
Does not change things though if your departure and or arrival area, people and or venues are not safe.
Its a system.
Boeing should stay away publishing results. Based on recent history (737MAX crash communication) people do not believe they’ll publish the truth if results looks real bad for their aircraft.
I agree that is valid, you parse the results and see if there is the spin wordage vs actual details.
Or they could do good work on small details and still put the company in jeopardy through their greed (per the bribe (errr dividend), ala borrow 13 billion to pay it so they can buy off shareholders to keep their jobs)
Some recent findings from Drostens podcast:
10% of infections are from (a) smear infections (touching contaminated surfaces and then touching your face).
The rest is evenly distributed to (b) droplet infection by larger particles that will sink quickly to the ground and (c) to infection by aerosol, which consists of smaller partcicles that can hover in the air for over one hour.
Infectious people generate both larger droplets and aerosol when coughing, speaking and even when breathing.
The aircondition can disperse aerosols to uncritical levels. I think MEL rules have to be changed under Corona conditions. Currently the AUX power supply is not in the MEL list. Meaning that on an aircraft with inop AUX power you potentially have no aircondition while the main engine is shut down. Parking positions directly at the terminal finger often have external aircondition support. But outer parking positions do not.
Pregnancytest-style quicktests can currently only identify some 70% of infections. That is noticable worse than with PCR test.
PCR tests are currently done with fluids grabbed from the very deep back of your throat. Thats both risky for the person poking into your throat and it takes time and many many poking sticks (supply is potentially sufficient). And imagine doing that before check-in for everyone.
Drostens team has recently compared PCR tests from spit (just spit out) to be only 5% less efficient using samples from known infected patients. So this would be a safe testing mechanism that doesnt take much effort to retrieve samples. I think analysing the samples will take an hour or two, however.
Good info and it cross checks with other sources.
I do have some adder and ponderings.
1. Spit Test: you are spitting into a container and then ship it off. Ergh. How safe is that? It like large droplets and humidity keeps droplets from drying up. It seems on the surface a better detection system but as bad or worse a vector of transmissions going through the mail and handling until at labs.
subset: Warmer temps (above 77) lend to a lower ability to transmit, but places like the US East Coast, South East, South, have high humidity. I have only seen some we don’t know on how humidity and other factors play in out in the real world. Brazil is seriously in trouble.
oddly, freezing preserves it despite the extremely low if not zero humidity in a freezer. Made that mistake to take frozen to frozen thinking best, now its a surface clean and or wash.
A/C: Those are complex systems and many have humidification setup (humid areas use it to lower humidity as the cold coils strips out moisture ). Legionnaire disease (bacteria so a different critter of course) hid in the wet and damp areas of those systems . So its a complex and may not be one answer but a more complex set of interactions.
MEL: If the AC breaks its not the power backup, its the AC unit itself that is most likely gone. We lost it going into Dallas one time (or one of the packs, not sure they don’t have two). Horrid hot the last 30 minutes – which prepared us for Dallas as it was 95 deg and 95% humidity.
Each engine has a generator as well.
To get me to fly, at this time, it would take: 1) Blocked off the middle seat on a 6-across single aisle; Blocked off middle and aisle seat on the two-side 5-across single aisle. 2) A plastic curtain between rows that comes down below and on the forward side of the seat backs. 3) All passengers wearing a face mask that covers their nose and mouth (no half measures.) 4) A slow boarding and disembarking. Why? Because that is when a passenger would be doubly vulnerable to infection.
Its going to take a proven Vaccine for me to fly!
Call it next summer maybe (though I may be in line for risk factors which I have 2, neighbor of which I had any control over, getting old and asthma. )
I think one of the keys to prevening transmission in flight is the venetilaton system. The airflow must be made to flow downward. Perhaps air intakes on the floor level annd vents that provide mostly filtered air for passangers. Maybe a UV strobe when people cough?