Leeham News and Analysis
There's more to real news than a news release.
Bjorn’s Corner: Do I get COVID in airline cabins? Part 13. DOD tests confirm OEM results.

By Bjorn Fehrm
October 15, 2020, ©. Leeham News: Yesterday the USTRANSCOM and its US Air Force Air Mobility Command (AMC) published the results of extensive airliner COVID infection risk tests. The tests, which were made to check the risks for DOD personnel using commercial flights, were made on United 777-200 and 767-300 aircraft in cooperation with United.
The tests checked aerosol dispersion of the virus in the cabins for both simulated flights and real flights. The result was you need to sit next to an infectious person for 54 hours to inhale a viral load that could make you sick (worst case).
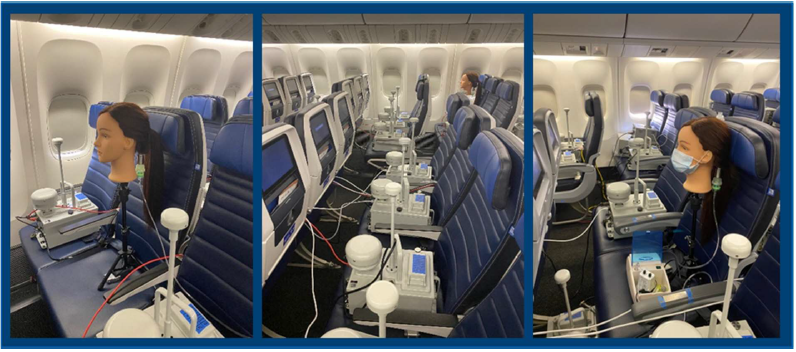
Figure 1. DOD tests in the cabin of United aircraft. Source: DOD.
DOD tests go beyond the OEM simulations
Last week we could report about simulation results from Airbus, Boeing, and Embraer. We also presented the latest statistics from IATA about actual flight infections. In Boeing’s case, we could say they had verified their CFD cabin simulations with actual tests.
Boeing supported the DOD tests with United. The results of the test are in the DOD report you find here. The US Transport Command did the test to understand the risks for their personnel when flying on commercial flights.
The report describes an elaborate test setup with a mannequin head as an index person and 40 IBAC (Instantaneous Biological Analyzer and Collector) samplers spread over the cabin (Figure 1).
The tests checked aerosol dispersion from 300 simulated breathing and cough events, using aerosolized viruses represented by microspheres of 1um and 3um diameter. A total of 11,500 breathing zone samples were collected during simulated flights (aircraft on the ground with air-conditioning on) and real flights at 35,000ft.
Tests were made with and without masks and with the mannequin breathing and coughing. The results support the OEMs’ results from last week. In many ways, it goes further than these as the DOD report includes a discussion and assumption of required viral load to get COVID from an inhaled aerosol.
Conclusions
There is a lot to get from this report as it’s concrete in its tests, its results, and the conclusions from the tests. Here the main conclusion in the Recommendations section:
For the 777 and 767, at 100% seating capacity transmission model calculations with a 4,000 viruses/hour shedding rate and 1,000 virus infectious dose show a minimum 54 flight hours required to produce inflight infection from aerosol transmission.
The report also states why it reaches this result:
The dispersion data (Figures 14-17) demonstrates the dominant protective factors, as tested, are the airframe’s high air exchange rates, downward ventilation design and HEPA-filtered recirculation and that other test conditions have measurable but minimal effects for aerosol risk. The dispersion data also shows that inflight, ground, and boarding conditions provide similar protection provided the air exchange rates are similar and maintained.
The extract mentions other test conditions, meaning gaspers are on or off and risks during ground and boarding conditions. The effects of gasper use are measurable but inconsequential. Hence gaspers can be used for personal comfort as required. The on-ground and boarding remarks are only for when you are in the cabin and its air stream. No tests or discussions are made for Jetbridge or Gate conditions.
These results are the same as from the OEMs. The cabin flow, including its turbulent parts, is very effective in dispersing and moving viral particles away from the passenger’s inhalation zone.
The OEMs have analyzed whether shields between seats, as proposed by cabin seat manufacturers, shall be introduced. All three OEMs conclude their positive effect is minimal and they have major other drawbacks for safety evacuations and in case of fire. The OEMs will not support the introduction of such devices.
The DOD tests should conclude the discussion about being infected while in flight. It’s time to turn the attention to where there are remaining risks, the phases before entering the aircraft, and when stepping out.
There are obvious risks in these parts that can be mitigated with disciplined behavior. Right now passengers are left without concrete recommendations for these phases of flights. Such are badly needed.
“The cabin flow, including its turbulent parts, is very effective in dispersing and moving viral particles away from the passenger’s inhalation zone.”
I think it would be more accurate to instead say something like:
“…is very effective in preventing the accumulation of a sufficient time-integrated inoculum of viral particles within a typical passenger’s inhalation zone”.
That aside: the gist of the conclusion is clear, even if it is based on a very idealized simulation of cabin conditions.
The real problem at the moment is that there is basically nowhere to fly to, due to quarantine-on arrival-schemes: if something can be done about that, then flights will start filling up in the morning. Singapore is thinking aloud about introducing a scheme that would remove the quarantine and instead replace it by a combination of:
– Mandatory pre-flight test;
– One or more mandatory follow-up tests during your stay in Singapore;
– Mandatory use of a tracing app.
I can imagine that countries such as Thailand may be considering something similar: their rainy season is coming to an end, the tourist season is starting, and tourism is hugely important to them. If Asia starts to unveil something like this, hopefully the rest of the world will follow suit.
With regard to testing, apart from the use of (slow) PCR tests, (rapid) antigen tests and sniffer dogs, there is now a newcomer to the mix: a laboratory in The Netherlands has developed a fast and simple breathalyzer test. When compared to PCR tests, it very accurately identifies non-CoViD-infected persons. It produces a relatively low incidence of “indeterminate” results, which require a follow-up test for clarification. A combination of such breathalyzer and antigen testing sounds like a very attractive candidate for airport use — both for outgoing and incoming passengers.
According to the NL breathalyzer developers:
The device will not be usable for the travel industry, says In ‘t Veen. “This device tells you how you are now, but not how you will be in a week. Therefore, when traveling you should still be quarantined when you go abroad.”
This is a not a flaw in the device, it just points up the difficulty presented by the incubation period of the virus. It would be useful to limit infection risk in-flight, but doesn’t get around the basic travel problem. And we know now that the in-flight risk is already low.
Hence the comment regarding the follow-up testing in the Singapore proposal.
The breathalyzer device is eminently usable…you just have to carefully define the goal of the test being performed.
Somewhat of an analogy can be made to temperature screening at airports. The purpose of temperature screening is NOT to give the certainty that everybody that passes through is CoViD-free: the purpose of temperature screening is to identify people with a fever. The interpretation of that result, and the attendant policy for dealing with it, are a separate issue.
This article reports on an interesting study showing that a single passenger infected at least 4 others, likely during the 18 hour flight. All infected persons were sitting within four rows of each other. The aircraft type was a 777, it had 86 passengers and masks were required and a pre-flight negative test less than 48 hours prior to travel.
The conclusion that the single case infected the others on the flight was done by genetic DNA analysis, confirming that 4 of 7 infected persons on the flight were infected from the index case.
https://www.stuff.co.nz/travel/travel-troubles/300165124/a-new-zealandbound-traveller-tested-negative-for-covid19-before-a-flight-he-had-the-virus-and-infected-4-passengers
Mr. Fehrm,
Thank you for an informative series of posts re Covid.
I would be interested to know if flight crews of freighters enjoy similar protections as found in passenger cabins. I can’t determine if my company’s converted B747-400 airplanes still have their HEPA filters installed when they were pure pax/combi birds, or if our new-build B747-400/-8F airplanes also have said filters installed as original equipment.
Thank you.
Don
The stakes are high. In terms of independency, OEM’s, airlines, IATA are not in the right reference group. Simple as that.
I would prefer a WHO / NTSB research instead of DoD/Boeing to be honest.
Based on observations, actions, learning curves, dramatic Covid-19 policy changes and reliability track records over the last 8 months.
While everybody was told there is no risk at all, OEM’s were extensive airliner COVID infection risk tests, in secrecy.
I would like to see the full report, assumptions, airflow and full conclusions iso abstracts & fancy pictures. As said stakes are huge, and massive perception management is all over us. While we embrace for the second wave.
Might be more accurate to say that the results were apparent from statistical data, but the OEM’s (and DoD) did their diligence and ran the studies to determine if there was a scientific basis. It now appears there is.
Bjorn gave the link to the full report, it has all the details. Experiments were carried out within aircraft on the ground, in flight, and within the jetways.
Does the link work? Not for me..
There are two links to the report, both work (just tried them).
@Keesje
I’m not sure what is the point of this flying is safe discussion, at least insofar as catching or not the disease is concerned
I do understand that a section at least of the ruling élite/gvmt, DOD no less, is prepared to go to some lengths to publicise safe airplane travel
I have not see similar initiatives/studies for trains or buses, perhaps some exist? The only pertinent bit of news I picked up is the NY transit system is wanting to implement a no talking curfew
A piecemeal band aid approach of safe solutions here and there would appear to ignore the necessity of an overall program – there is little long term point in travel if the place you are going to lives in such uncertain health as where you live, with correspondingly restricted lives, and cleaner countries are hardly likely to welcome health refugees, unless used to importing the very rich, like NZ
The overall progam, in the west, has been a number of badly managed serial lockdowns : plan b’s seem rare, unless it is the ‘race’ to create a vaccine, unlikely to come effective and quick, the distribution and uptake of which requiring far superior PR, administrative and logistical skills than so far shown in US or EU
This is part of a wider failure, administrative, political and economic, perception of failure and mounting distrust of ruling élites not only within the US much more so without
To impose masks social distance inessential/essential ‘frontline’ lockdowns curfews, the war language – all this is victim blaming
The structure of all aspects of community life should be resilient enough to withstand events like this virus, the appearance of which has been foreshadowed over the last twenty or more years and the means of production of which are evident in ind ag
One can say the means of production are deliberate, given that the same conditions (essentially health care) are applied to humans as they are to animals, in ‘rich’ industrial societies in the ‘west’
It is absurd to treat people as a herd, to impose industrialised living conditions and drug regimes, then to wish for unquestioning obedience/compliance in the adoption of responsible middle class style actions such as social distancing and the wearing of masks, in circumstances where these are close to impossible among the poor but easy among the rich
To advertise tiny industry by industry solutions is to suppose that by increment by application of advanced technologies an overall program of making life ‘safe’ once again is plausible and possible and is even under way ; It is not
To discuss this subject is a distraction from discussing a general solution to this dilemma
Not sure if you watched the New Zealand political debates, but they stood in stark contrast to the US debates. A packed audience with people sitting side-by-side, without masks and without fear of infection. Candidates sitting next to each other.
It was like a different universe. Nice to know that it’s still possible. It also puts the lie to the case that such progress is not possible. It was achieved by following the science, instead of denying it.
Europe “followed the science” also.
Easy to achieve success when you’re a small, sparsely-populated, very isolated island group with a relatively minor economy. Try that with a large, densely-populated, thoroughly-connected economic hub with a land border thousands of kilometers long…and without a totalitarian Communist party in control. Even Australia is having a very hard time trying to emulate NZ’s success…even though it too is an island.
So console yourself that, even with another administration, the US would still be in a pot of stew…just like most of the rest of the world. If you want to explain the relatively high CoViD mortality in the US, don’t forget to pay due consideration to the significant obesity problem there, and the rather elitist healthcare system.
The reason for New Zealand’s success is that the people ultimately followed the policies of the government, which were based on the science alone. Not on what people wanted or complained about. Just on what worked.
They had their own population of naysayers, but they were a much smaller minority. In the US, we have the president as naysayer-in-chief. Impossible to get the same results in that environment.
Maybe as non-island nations, we could not get down to the same levels as New Zealand. But for sure we would not be seeing the oscillating waves we have at present.
Look at the Rt curves on rt.live. Any engineer would recognize that as the ringing response of an underdamped system. Then look at the curve for New Zealand, it’s a critically damped response, with one ring. Who provides the damping? A combination of the government, through effective use of policy, and the people, by willingness to follow the policy.
Also, Ardern has recognized the sacrifices people made to comply, and has praised them and given them credit for the success. She knows it wasn’t easy but she also knows they now see it was necessary and effective. So she just won in a record landslide, because the people support her.
At a recent COVID press conference in NZ, an American student got up and asked for proof of the virus existence. He was immediately sat down and dismissed. No room for that kind of BS in their discussion.
Would that we could do that here. Instead, we have bloggers, tweeters, and prominent politicians pounding away that masks are ineffective, COVID is a hoax, vaccines are a conspiracy, etc. Anything to deny the truth and the science, and to elevate their personal opinion over the facts.
@Bryce
To praise and to wish to reproduce the until now apparent success of NZ is to ignore reality
Countries are very different, in most aspects, and one size fits all is not going to work, and has not worked
In fact this ‘if only we could be good like NZ’ fantasy results from the same illusion that there is a ‘science’ or ‘technical’ solution available, only that people and gvmts are too….your choice of word for stupid .. to accept this or these solutions : a train of thought leading straight to a dead end
In this similar to the quest to prove that airtravel is safe, tick, metro travel next, tick, then lets solve living in houses….
Unhappily for NZ this bug, and those to follow, is unstable, mutates, and is plentiful everywhere in humans and animals around the world
Long term isolation will hardly be palliated by the most efficient of vaccines, if ever these are invented
As with all problems – best to go back to the beginning, where and how does this virus emerge and spread from animals to humans, and how might this process be staunched or stopped
@Bryce PS Useful link
https://critinq.wordpress.com/2020/10/16/an-era-of-pandemics-what-is-global-and-what-is-planetary-about-covid-19/
Gerrard, you persist in both denying the science and the results of the science, and the consequent belief that nothing can be done. Mankind deserves the pandemic because of science and industry. Until the influence of these are destroyed, we will have recurrent pandemics.
All is hopeless and a vaccine won’t work either. Those who believe in/look for solutions are engaging in fantasy and/or are stupid. The path of understanding and action leads to a dead end. If progress is made, it’s only illusory.
That’s all fine, it’s your opinion, and you have a right to express it here. But it’s solidly refuted by the evidence before us, NZ being only one example.
@Gerrard White
You addressed 2 of your comments to me, but I think you meant to address them to Rob?
Rob is the big fan of the situation in NZ…I’m not so sure that it’s a (long-term) success story. Just this morning I read that there was a new incidence of local transmission in NZ…in that respect, they’re living on a knife edge. I’m reminded of the horrendous flare-up that occurred in Singapore, after its initial stellar succes. I’m more impressed by the Swedish approach.
@Rob
I do not deny the ‘science’, I say that the piecemeal and inefficient application of such, in the west, has failed
If you care to take a look at what the ‘science’ says about the production of viruses you will see that steps can be taken to diminish and prevent this – read the link provided
Look also at predictions, by scientists, concerning the likely effectiveness of a vaccine : combine this with reports concerning likely vaccine uptake
Piecemeal solutions are comforting, perhaps, but they will not add up – so the plane is clean, is the house, the factory, the farm?
You appear to think that the west is slowly getting the ‘science’ together and will eventually find an overall solution; one which appears to have, largely, been found, by many Asian countries already
Ask yourself what elements were effective in Asia, and why the west incapable and ineffective
You will find there is more to ‘science’ that you suspect, and that the ‘science’ used elsewhere was well used whereas…
I am not hostile to science, just to your version, which does not work, or which you are unable to get to work
It’s mostly a matter of political execution. I have been critical of the West in terms of not being able to generate the desired response and behavior in their populations. Authoritarian governments have an easier time of this, but it’s not impossible for a democracy, as the example of New Zealand has shown.
I just don’t confuse a failure of execution with a failure of the underlying scientific principles. Political freedom means the right and ability to dissent, and to conduct civil disobedience. When that is done over political or philosophical issues, a democratic government must adapt and factor in the viewpoint of the dissenters, or face escalating consequences. Or they can behave in an authoritarian way and put down the dissent by force.
However the foundational assumption is that reality will feature prominently in the thinking of all sides. If the civil disobedience is over the earth being flat, there is no accommodation by the government that can make that happen.
Similarly if it’s over the denial of scientific evidence or fact, the effectiveness of masks or other protective measures, the death toll for natural herd immunity, whether the illness can be fatal (for others but not for me), whether a vaccine can be effective, the government should not accommodate those views.
In the West, we see that sometimes it is the governments themselves that hold those views. That is a breach of their responsibility to the public, but they’d need to face reality to understand that.
In Sweden, the response of the government was to follow the science, accurately inform the people, and rely on them to make good decisions. That was effective except in the initial case of vulnerable populations, which suffered excessively at first, but then Sweden took measures to better protect them.
As in New Zealand, success depended on the population accepting the government policy and following it. A difference with New Zealand was that Sweden did not attempt to drive the transmission rate to near-zero. That may not have been practical or achievable in their circumstances. As it happened, it was for New Zealand.
But my overall point is, if the science is followed and both government and public accept that, the consequences of the virus can be limited. That requires common perception and cooperation by government and public. It can be forced by an authoritarian government, but that is by no means a prerequisite.
In a democracy, more than anything else, it requires education in the science, as well as objective thinking. If either government or the public abandon those values, then the execution will be poor. That is what we see today.
@Rob
‘Following the science’ can not be the number one priority
Priority- Enquiry as to causes of the virus as well agreement building as to how to modify the means of production and reasonable measures to relieve the disease may be taken
In the vast majority of cases, countries, in the west, the measures taken by various gvmts were if not unconstitutional were taken under a state of emergency declared
Such emergency powers, rather than initiation of any democratic procedures of decision, were made necessary by the fact that neither gvmts nor health experts had taken any measures of preparation, despite many warnings over the last 20 years, and had no idea what to do, and panicked
As the link I quoted makes clear, it is not as though the production of such viruses has not been known for a long time – neither ‘science’ nor anyone or anything else took any steps to reduce risk
If ‘science’ has been first ignored then deployed with such incompetence – why should you expect respect for such?
It may be seen that improvements to the understanding and application of ‘science’ can only be social/political – moreover compliance, essential in social diseases, can only be voluntary, over the long term at least
‘Science’ does not exist in another dimension apart from such context – successful adoption of priorities depends on recognising such – imposition will not work
As for NZ – over time isolation will become intolerable and will of itself fail to continue to protect from the virus entering the country, the bug can enter in many ways, in animals and food and …well we’ll find out
At some stage their infection rates will have to fall in line with those prevalent with the rest of the world, or they will remain in isolation
There’s no point in stamping out a fire in one very, very, small room if the house is burning down
This is globalisation- To reverse it on your own by yourself is to try play the hermit in Disneyland
@Bryce You are right, I wished to be un contestarian in so doing but…..
I do not think, neither do some WHO people, that NZ can survive long term without getting the to the same incidence at the rest of the world more or less
Sweden is viciously criticised for their open minded and consensus oriented as well as un hysterical policies – by critics from democratic countries outraged by this exercise in democracy found to be working
Attempts to extinguish or eradicate this bug are a lost cause, better to to learn to live with it, and look at altering the conditions of production
Gerrard, you have your own unique point of view, but it won’t govern the actions of the world. People will try to deal with the virus, and however poor the execution is, will not stop trying.
Hopefully they will learn and do better over time. Some are already doing quite well, no matter how much that is denied. This crisis too shall pass, as all things do, and as previous viruses have.
@Rob
You state that people are trying to deal with this crisis
I am pointing out they are perhaps addressing some of the known symptoms, but they are failing to address the problem
There is no point in a clean NZ or plane, that’s taken 8 months and is hardly definitive how long is cleaning up the rest of the world going to take?
There is a point in realising that solving a problem means understanding that it is not solved by palliating symptoms but by curbing the conditions of the production of the problem
Otherwise this bug will have a long number of successors, and every time we’ll get a fresh DoD report on how it is safe to do this or that
By the way this is the same DoD that’s been winning that war in Afghanistan for twenty years or more, they obviously like winning wars so well that they can not stop
This is not the sort of mentality best equipped to problem solving, in fact it is the opposite
It appears Donaldson HEPA filters are OEM for the B747-8F and Intercontinental. I would assume they are on new-build –400Fs but I recall the filters were removed from some -100/200 P to F conversions.
Hopefully airflow in freighter cockpits coupled with mask use will minimize Covid-19 transmission.
To the best of my knowledge, only one cargo crew reported Covd and was confirmed.
It not like it cannot happen, but the risk is low and the cargo crew contact are very limited.
Very low per the real super spreader events.
At my airline management is not telling us how many crew are infected, nor how they are thought to have become so.
I would estimate less than 5% of our crews wear masks while together in the cockpit in flight. While speaking to my FO pre-Covid I noticed flecks of spittle that flew out of my mouth in the bright morning sunlight coming through the windshield, and I’ve never considered myself a ‘sprayer’.
People choose to ignore masks at their peril, which would be fine except they are going to take a lot of innocents with them. And destroy the very economy they purport to want to ‘open up’…
Hmm, 1000 virus = infective dose. I had never seen this quantified before. Is it an assumption? Or supported data point?
I have never seen such figures either.
In fact, just a few weeks ago, I heard Dr. Fauci explicitly saying that nobody has any coherent information on the link between the size/duration/nature of the inoculum and the resulting extent of infection.
It strikes me as a (quasi-)educated guess.
The report says that studies vary as to the precise load, and also it varies with the individual. But this is an average number within the range of previous studies. The references are given in the study if you want to research further.
It is the bording and debording that can be a problem, airline routines how to avoid crowing during these moments is the key and ICAO/IATA should come up with optimal regulations with approved procedures and maybe full throttle ventilation running on ground power during at these moments. Airports could modify its ventilation systems to have the same downdraft from security to bording tunnels to qualify as Corona safe airports.
This has been our point since the spring when the low risk of the flight seem probable but the other risks were real and un-addressed. Still, nothing is done by IATA who is the correct body to address this.
The Airport Council International (ACI) introduced an Airport Health Accreditation (AHA) program in July, which sets airport standards for adaptations to COVID, to help protect passengers. Airports can apply and are evaluated according to the ICAO CART recommendations.
Numerous airports are now accredited, with more joining every week. There is an Apple smartphone app that lets you see airport status, and for those airports that are accredited, allows the Check & Fly feature to provide airport & airline specific information to travelers. This feature will be available as a web site eventually.
Perhaps this would be one of the groups to approach about the non-flight issues with COVID exposure to passengers?
Thanks, Rob.
This concerns the airport, where the airport authority is in charge. The boarding procedure, from the Gate check of the ticket until you are in the airplane and back again at the destination is where the airline is in control. And IATA is the airlines’ central agency. I want IATA to act and issue comprehensive recommendations.
I have zero faith in IATA, its a committee with all it inherent flaws.
Regulators taking aggressive actions works. A committee that is all about compromises will never be effective.
Thanks Bjorn, I agree. If there was an IATA COVID accreditation program for airlines as there is for airports with AIC, maybe that would help to enforce best practices as recommended by CART. Maybe that idea could be put forward to them.
Is there any scientific prove passengers got infected during (de)-boarding? Maybe they were infected elsewhere. The airflow during boarding deboarding is vertical and even improved if cabin doors are open. This will only slow / complicate the process, meaning people are in the cabin longer. (Which is no problem because it’s safer than most places)
Not my opinion, but this how risks are rationalized away these days.
Patrick Ky said today that EASA will issue their RTS AD next month and allow a 28-day comment period. They are aligned with the FAA, so the MAX should be cleared to fly by the end of the year. Other regulators are expected to follow.
Some good news for Boeing as a company and the employees. The organization is still undermined by what has to be the worst mis management in history.
The depressing part is that two aircraft crashed after the engineers did a stunning job on keeping an old design competitive, because of a single fatal flaw.
Downside with engineers, give them an impossible mission and they can figure out ways to do it. What was intended as a get us through fix becomes the solution.
Much like the Kansas city Hyatt Regency catwalks, nothing wrong with the design, the execution failed (though in this case I would put it that it was changed at the engineering level to created the failure)
So just because you can make something work, should you?
France is introducing fast CoViD testing at airports before the end of October:
https://www.britishherald.com/rapid-covid-19-tests-to-be-introduced-in-french-airports-this-month-says-minister/
Thanks Bryce. It appears that initially this will not replace the quarantine policies, but if the testing shows that it accurately predicts the results of quarantine, then it could do so in the future.
This would be very welcomed by airlines and airports, if shown to be effective. Another key requirement would be for it to be accepted by most countries for international travel. So everyone will be following this with interest. It’s good that France is willing to try it.
On the subject of CoViD vaccines, a Sinovac vaccine was administered to (volunteer) residents of the Chinese city of Jiaxin yesterday, before Phase III trials are completed but after emergency use authorization was granted by the Chinese authorities. Those participating were charged the equivalent of $60.
https://www.businesstoday.in/sectors/pharma/chinese-city-offers-sinovac-coronavirus-vaccine-for-emergency-use-at-60/story/419154.html
It’s interesting that people are willing to pay in order to be a guinea pig. The people interviewed on TV yesterday had infinite and unconditional faith in the vaccine, because the authorities “had told them that it was safe”.
Dear Mr. Fehrm,
How do you explain the SARS-CoV-2-infections on flight VN54 from London to Hanoi on March 1, 2020?
“Studies trace COVID-19 spread to international flights
…
Of the 16 crew members and 168 passengers tested, 15 (8.2%) were positive for the novel coronavirus, 12 (75%) of whom had been seated in business class with the symptomatic passenger, for an attack rate of 62% in that section of the 274-seat plane.”
CIDRAP, Centre for Infectious Disease Research and Policy, 21.09.2020
https://www.cidrap.umn.edu/news-perspective/2020/09/studies-trace-covid-19-spread-international-flights
There are two other studies mentioned and concluded, that “”SARS-CoV-2 test results have been positive for hundreds of flight attendants and pilots; at least 2 have died. … Our results demonstrate that SARS-CoV-2 can be transmitted on airplanes.”
If this report has been discussed before, my apologies, I couldn’t find any reference to flight VN54 via the search function.
Thank you
The problem with these reports is they make no effort to separate airport, gate, boarding, flight, deboarding, gate, airport. They just know the person flew from London to Hanoi with an index person and got COVID in the aftermath. What we have convincing research showing is that the flight phase in itself, with masks (1 March is before masks) is safer than just about any other public environment. This doesn’t mean going on a flight is safe. As we have pointed out from the start it has several risk moments that are not in focus because the human brain focuses the sitting beside someone with COVID. We are stuck and can’t move, hence it’s risky. We and the airlines should focus on these remaining risks; gate queue, jetbridge or bus trip to the airplane, boarding, deboarding, jetbridge/buss again, gate.
Crews are especially at risk as they leaned into the passenger row, meeting the passengers breathing face to face. Initially breathing was not considered a risk, only coughing and droplets. Today we know breathing and aerosols (small droplets that stay airborne in poorly ventilated spaces for hours) are as dangerous. When the pax has a mask the risk goes down significantly (the DOD study shows more than 5 times) and a masked Crew reduces this further. But crews have stopped leaning into passengers breathing area for this very reason. It’s their workday exposure and they should be careful.
It’s notable that although these studies are recently reaching peer-reviewed publications, they all reference events that occurred at the beginning of the pandemic, before the risks were clearly understood. If you look at the extensive history now available of results from flights where precautions were taken, you don’t see any pattern of significant transmission, either among passengers or flight attendants.
This also mimics the initial experience of hospitals and nursing homes. Before the risks were understood and precautions taken, there was significant transfer between patients, and also to healthcare workers. It was far worse than aircraft as there wasn’t the same protection of ventilation rates, However with learning and precautions, the transfer rates are greatly reduced and for healthcare workers, less than the general population.
One of the benefits of Bjorn’s series has been looking at the big picture and all the available information, not just at studies that favor one or the other position. That has differed from much of the general press coverage which focused on the same few studies from the original SARS, and now perhaps studies from the beginning of the pandemic. Also the focus has been on the science and how we integrate our scientific knowledge with the observed results.
Did the simulation include passengers taking off their masks to eat meals and drink fluids? How was the lavatory sanitized during the simulations (assuming they were used)? What about 6 foot social distancing when boarding (I would like to see how long that line would be in the airport
The point of the study was to establish a scientific basis for the observed low statistical rate of transmission in aircraft cabins. So although those behaviors were not simulated (the study explains the reasons), they’d be unlikely to significantly alter the results.
Most time in an aircraft is spent seated with mask on. The study shows a significant margin for that case, before infection would occur. The margin would be proportionately reduced for time without a mask.
We know from the statistical evidence, that the risk is low in real flights when these behaviors are present. We know from the study that the reason is insufficient viral load transference for infection. That provides an understanding of the observed results.
Interesting article on Reuters today, in which a number of experts distance themselves from the recent IATA/OEM presentation regarding infection risk:
https://www.reuters.com/article/health-coronavirus-airlines-risks-int/bad-math-airlines-covid-safety-analysis-challenged-by-expert-idUSKBN27412C
The risk is still low…but most likely much higher than the fantastically low numbers presented in the report in question.
@Bryce
Thanks, sanity does exist – the figures originally given by the OEMs and essentially confirmed, I think, by the DoD report, are blatant PR ing
This sort of report gives the industry a bad name and, one can suggest, alarms rather than allays potential pax
Does this not rhyme too cheerily with the Max is safe chorus?
Triggered by this “recant”, the DoD would do well to do a new study, this time with:
– A more realistic number of infected persons on board, e.g. 5-10.
– Movement of persons around the cabin.
– Particular attention to persons seated adjacent to the lavatory doors, and the entrance/exit doors.
– Unmasked children on board.
– Removal of masks for eating and drinking.
Methinks that the outcome will be a lot less rosy.
It’s notable that the objection is based on the uncertainty created by the fact that, not every person being counted as a non-infection, was tested and verified as non-infected. So in that sense the number of positively non-infected is in fact unknown. We only assume the lack of reporting implies non-infection, and we only know for certain those cases that were confirmed infected and traced, which is a very small number.
That uncertainty exists and is valid, but once again for the conclusion to be untrue, there would need to be large numbers of infections that were not traceable back to a flight. That is where the 1.2B global and 214M US numbers become significant. It’s highly unlikely that within that extremely large sample group, there would not be more instances found, if the transmission rate was significantly higher, But that is not what we find.
So in that frame of reference, the absence of evidence is actually evidence of absence. I get that some of the researchers feel that their work was co-opted for a conclusion they don’t endorse. I don’t fault them and they have a right to object.
But at the end of the day, there is not evidence for their concerns, there is only concern that evidence has been missed. If anyone can establish that evidence, it would be an important finding that would alter the conclusion.
Rob, sometime research proves too incomplete to publish, boasting incorrect perceptions. We need to be objective, strong and brave enough to admit that. How many of the 1.2B people were tested on Covid-19 within a few days of their trip, can it be linked to their flight. Skipping those considerations & high lighting a small incomplete part of test results, is indeed giving the industry a bad name.
I warned before, this is OEM’s, airlines, IATA, not independent at all & the stakes are high. It would have like WHO & e.g. NTSB publish research on this.
the Dr who performed the study refused to participate in the BS spin the Govt and Airlines want to put on his study.
he cites the fact that of the “1.2 billion passengers only 44 contracted COVID on the plane” as a false narrative because only a very tiny fraction of those 1.2 billion were tested or in any way contact traced.
as he says, absence of evidence is not evidence of absence.
https://jalopnik.com/study-finding-it-nearly-impossible-for-airline-passenge-1845427485
dr Who? you’re kidding