Leeham News and Analysis
There's more to real news than a news release.



Bjorn’s Corner: Do I get COVID in airline cabins? Part 11. Wrapup.

By Bjorn Fehrm
July 18, 2020, ©. Leeham News: It’s time to wrap our Corner series about flying during the COVID-19 pandemic.
We started the series on the 8th of May. A lot of knowledge has been gained since, about COVID-19 in general and when taking a scheduled flight.
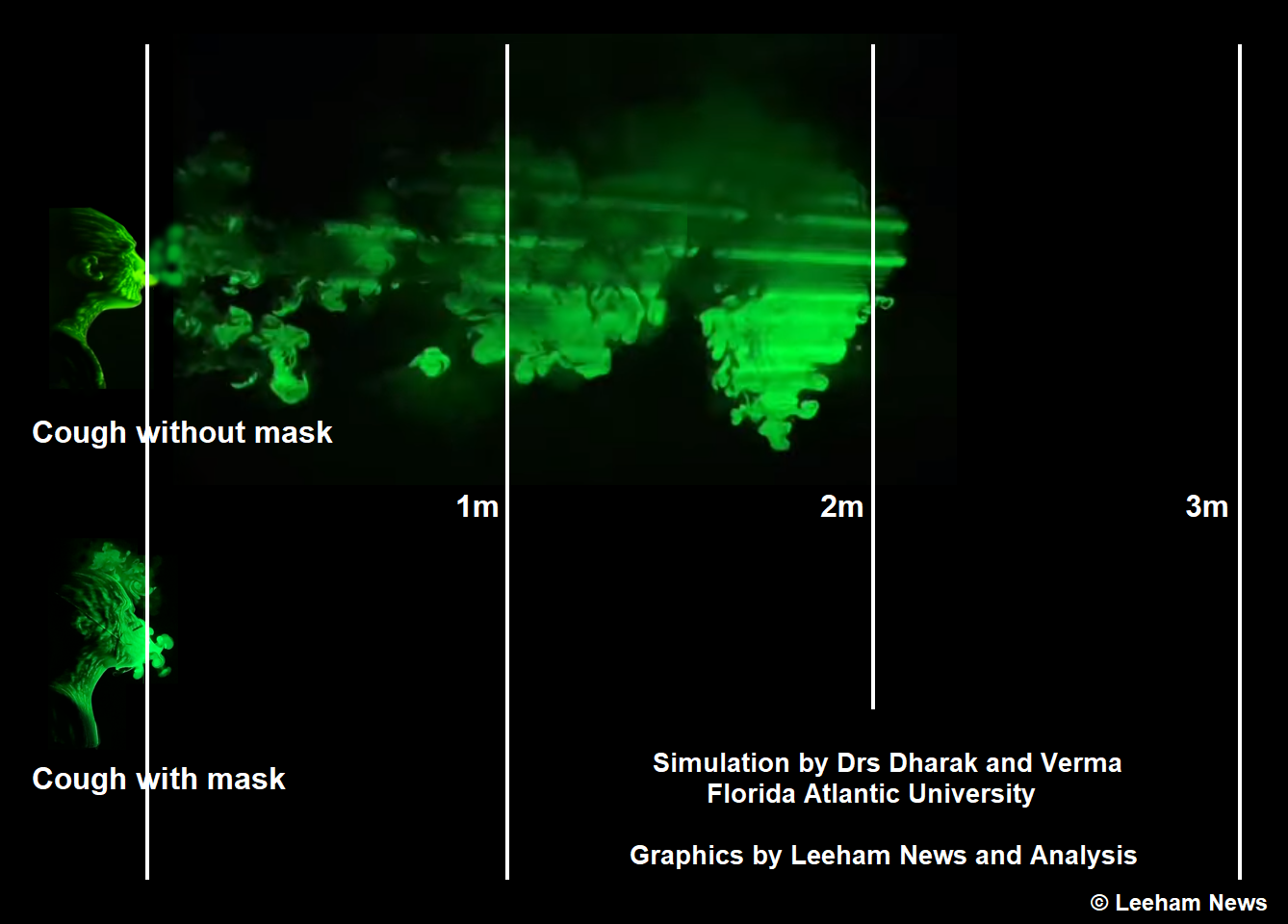
Figure 1. The difference of coughing without and with a mask. Source: Simulations by Florida Atlantic University, composited and annotated by LNA.
What we learned
In the first Corner, we showed the dramatic difference in the reach of a cough exhale with and without a mask, Figure 1.
Since then, the risk of airborne transmission of the virus through droplets and aerosol has been confirmed by study after study.
The touch path, on the other hand, has not got any confirming studies. I haven’t come across a study that presents the probabilities for getting COVID-19 through a touch scenario.
The other fact that has been verified is just how many that spread the virus without knowing it (asymptomatic spreading). You are infectious two days before first symptoms and the peak is the day before you feel the first symptoms.
The consequence is wearing a mask to protect others in indoor public places is now mandated by a majority of countries.
Where I live (France), we were down to 4 new COVID cases per day and million people, but it has in recent weeks grown to 8. The President has, therefore, declared masks mandatory for all public indoor places and transports (was transport only) from next week. If you don’t comply, the fine is 250€.
COVID and Flights
Surveys around flying during the pandemic have revealed people are most concerned about sitting beside an infectious person during the flight.
I have found no evidence that confirms this fear, for flights where the airliner was equipped with an Environmental Control System (ECS, Figure 2) with a modern HEPA filter (that stops 99.9% of germs included SARS-cov-2).
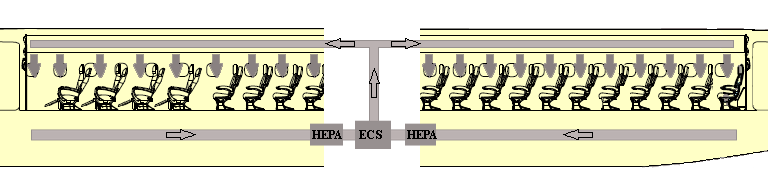
Figure 2. The air conditioning system in a jet called ECS. Source: Leeham Co.
Many make reference to a 2003 flight with a 737-300 were a virus was spread, but it’s doubtful this old aircraft had a HEPA filter of this type.
There is convincing evidence of transmission for indoor poorly ventilated areas. This applies to several parts of the boarding and deboarding process. We know from persons that have traveled recently, airlines have a job to do here. Several are sloppy in their procedures or have none at all. This is strange as they advertise extra cabin cleaning efforts etc. Is this for the show? Don’t they research where the real risks are?
We also learned you need a certain critical load of the virus to get COVID-19, as our first line of defense, the respiratory tract mucus attacks the virus as it enters. To keep your mucus fit it shall be kept hydrated. Drinking water during flights is more important than ever.
Flying has increased rapidly in the last weeks as countries have lowered restrictions. But the first signs of backlash are there.
We have flights where several deboarding passengers have tested positive at the destination. As a consequence, positive passengers are put in quarantine and restrictions are coming back.
For international flights, such events create havoc. The only change that can help international air traffic, besides a vaccine, is testing at check-in. With so much at stake, it’s strange this hasn’t happened. The technology is there.
Thanks again Bjorn, for this series. The two issues are the risk of infection during/from travel, and the risk of travel distributing the infection between locations.
The first issue, of risk in the act of travel itself, seems to be low. For 2020 thus far, about 1.2B passengers have been boarded globally. Conservatively, perhaps 250M of those have been post-COVID. Yet there are still very few reports of infections being traced to the act of transport itself.
If infection clusters begin to develop associated with the act of travel, then this could change. Although we have not seen that thus far, I agree that more could be done by airlines to ensure that result, without compromising their economic models.
The second issue of transporting infection, is more difficult. Unless nations work to hold down their rates of infection, it’s going to be a thorny issue. The only real solution, as you mentioned, is testing prior to departure. Testing on arrival is problematic at best.
Even that is not foolproof, and requires new infrastructure. The tests have to be for active infection rather than antibodies from previous infection. If a vaccine arrives, then the focus could switch from testing to vaccination. So the value of an investment in infrastructure would depend on the likelihood of a near-term vaccine.
Several countries are now requiring test before departure. Perhaps if the infrastructure becomes necessary to support this, in the absence of a vaccine, it would become as ubiquitous as TSA. Travel health/vaccination screening may be the ultimate result of the COVID crisis. Possibly there is value in this being established, even with a vaccine, in case future viruses arise.
I agree that testing before departure is going to become more popular.
That having been said, it’s interesting to note that the currently-used nasal/throat swab tests have a 30% false-negative rate, because of the difficulty in obtaining reliable swabs (even for medical professionals). Let’s hope in that regard that a more reliable saliva test (spit test) becomes widespread.
Moreover, for people who don’t have respiratory symptoms, it can be expected from the outset that a throat/nasal swab will not reveal the illness. A significant sub-group of CoViD patients (up to 25%) develop gastro-intestinal symptoms rather than respiratory ones, and yet there is no “standard issue” fecal test for such patients.
I’m not trying to be negative here: I’m merely pointing out that there’s still a LOT of work to be done to provide (more) reliable testing.
There are 3 types of tests, PCR and antigen, which are genetic tests for the presence of the virus, and antibody which look for the body’s response to the virus.
The PCR test is nearly 100% accurate but requires the uncomfortable deep 8″ nasal swab. The antigen test can use the lesser 3″ swab, but needs a lot more virus for a positive test, so can have a false negative rate of 20% to 30%.
The accuracy and applicability of the antibody test is still not well understood, because the body’s response is not fully understood. So it’s viewed as the least reliable, and is not a diagnostic test.
The other issue that occurs is timing. The PCR tests are most accurate 8 days after exposure, with the virus beginning to replicate in large numbers after 5 or 6 days of incubation. So there can be an offset of a few days between the contagious window and the accurate testing window. Note this is not a binary result, it’s a probability distribution that peaks at 8 days for most people.
Also the PCR test will continue to be positive for at least a few weeks after the initial exposure. In some people it can be a month or more.
So all these aspects would need to be factored into any travel testing regime. It wouldn’t be a perfect system but it would probably catch the majority of active cases.
1. There is a way of looking at this question as now meaning that passengers have now become ‘dangerous goods’ that need appropriate and consistent regulation worldwide. Some are dangerous, some aren’t.
2. Your excellent analysis concentrates on the facts as far as known. The return to the skies will require passenger perceptions to synchronise with the facts, which inevitably will include some probabilistic elements on the whole journey path (inclusing destination stay).
3. Those false negative rates from testing even if done rapidly are pretty worrying.
Just a comment on the masks: Many medical grade N95 Respirators have a outlet valve that does not filter the breathing out. It is to make it easier to breathe. Since they still are very hard to breathe in, you breath is much heavier. I was on a flight an saw that around 20-25% of the passengers were wearing these masks. And they are useless for stopping cough etc. I think use of these masks by health care workers that themselves had the virus and not knowing is part of the quick spread in hospitals and elder care homes. So these types of masks that only protects the user (if worn properly and you have shaved in the morning) but not stops cough etc should not be used. If they are used by the public indoors or in public transport then the mask use is useless. As they were worn they are not protecting the bearer and they are not protecting other people. Personally, I try to keep the 2m (or 6 feet) distance and do not have a face mask. I think that face masks in public gets people sloppy, and they do not keep the distance. I do agree on mask boarding and deplaning an A/C though and in public transports.(which I would avoid, own car is always better for a lot of reasons). But should be simple masks only to protect others.
Just to clarify, medical grade masks do not have a valve. The valve is found in industrial and worker masks, where the protection is meant to be from inhaling airborne materials. So this is probably due to shortages in some places, as well as public confusion about masks in general.
In my area, stores are now separating the two and there are clear signs about which are COVID prevention masks. In some areas, the valve masks have been banned for public use.
But they are still available including on-line, so no doubt people will continue to use them inappropriately.
This is an excellent point! This N95 with outlet valves are useless in preventing the user from infecting others and the public should be made aware of this. Where mask wearing is mandated they should be banned. Airlines should not allow these masks. There needs to be more education on this.
What is beyond stunning is AK has 50-70 some a day (since the lift of restrictions) with a population of 750,000 compared to Bjorn and France of 8 and they have put in mandatory masks.
The Muni of Anchorage has made them mandatory.
Truly tragic is that is a party thing for the lack (one of the best initial reactions equally depressing).
While I have nothing against France, I never thought it looked better than AK.
I fly in and out of Anchorage a lot.
None of our admin/ground staff were wearing masks at the end of June, with the exception of a couple mechanics. I had to insist the woman catering us leave the airplane and come back with a mask.
I think there is a false sense of security in AK, also a lot of people seem to feel that not wearing a mask shows they support Trump. In my home town in ‘liberal, enlightened’ CA mask use is spotty, at best, I think for the same reasons.
Going to be really interesting this fall, when ‘flu season cranks up. Salt with anti-vaxxers and stir in scientific ignorance; a fine recipe.
@Bjorn
Your report is fine for the plane
Although you do avoid the social distancing issue, which may or may not be necessary/useful in a plane, but has said widely to be imperative, if not paramount
There are two points –
Who and how is going to mandate and co ordinate the precautions and measures you suggest or those which will find wide consensus?
You do not mention measures in airports : presumably testing will take place in airports not in planes – so that after testing one is exposed to risk – it would be necessary to implement safety measures anyway
All this, knowledge and consequent measures – is provisional – treating the symptoms not the cause
The context – if the bug is circulating widely (as now or more so) across most countries successful protection in the plane will not have any impact on quarantine or travel policies
So – what will? How will international travel restore?
It appears that in Europe the lesser of two evils has won, for the holiday season at least, the day
Flights are subsidised and quarantines abandoned
In those areas that require testing for departure, the test is not done at the airport, but the person must present proof of recent testing. There is also a check for signs of current illness during screening.
Social distancing as a static measure is not especially feasible for public transport, beyond the ad-hoc method of using the available space around you. Good ventilation is also related to social distancing.
High ventilation would permit closer spacing while poor ventilation would require additional spacing. So sitting in an outdoor stand with others, or in an aircraft, would not be equivalent to sitting in a bar with the same spacing.
A consensus has been building in some areas, for example in the EU there are accepted common rules for travel. But there is a lot more work to do in terms of harmonizing and establishing prevention goals around the world, including the US which has lagged behind.
Can’t we SEO or digital footprint the passenger to determine risk? A group of 20 really shouldn’t be travelling together and if theg so, must be spaced father apart.
In Singapore, it feels like the vaccine to the virus is.. exercise. Or rather, keeping oneself strolling, walking or even pushing the stroller. We are getting Dengue though and despite wintery temperatures, nobody’s really reporting sick too.
International travel may never restore. It can’t either. I’ve bad news. We Asians are a lot more now. A lot more. Such population density was never going to work on open skies policy. And believe it or not, international links are not the the consideration.
It’s demand as perceived by NDC. China Southern fares keep surging 1,000% to 2,500%. China Eastern wisely avoided it: followed Air Canada to launch flight passess, and then to encourage onward travel, packaging them as Thank you parents flights.
Not surprisingly, Beijing Daxing, Guangzhou Bauyun T2, Shenzhen .
No social distance on board flights. Now Zhengzhou has A380 level demand that China Southern has sourcing.
We learned a lot. Maybe there’s more we can learn.
I learned there is no proof people weren’t infected onboard aircraft. Maybe because sick people didn’t fly, almost nobody flew. Infections are hard to measure anyhow. Is that encouraging?
I learned cabin air circulation is very turbulent. Even upwards in some places. Ceiling to floor is an eufemism.
I learned a volume of air, equal to the cabin, passes through the HEPA filter every ~3 minutes. To state the air in the cabin is refreshed every 3 minutes is close to misleading.
Sitting close to many people for a long time isn’t a good idea when a virus goes around. Aircraft are no magic exceptions. People are smart enough to understand. The basics. Unfortunately?
Aircraft cabin air is 50/50 outside ventilation and recirculated interior air. The total ventilation rate is equivalent to a cabin turnover every 2 minutes. With the 50% mix the theoretical turnover is every 4 minutes.
This does not mean that every molecule of air is evacuated from the aircraft within 4 minutes. There is turbulence and mixing, so you end up with a probability distribution.
Probability within an air mixing environment is well understood, from the principles of humidity control. For a bulk turnover period of 2 minutes with 50% mix, the reduction is 1/2 at 2 minutes, 1/4 at 4 minutes, 1/8 at 6 minutes, 1/16 at 8 minutes, 1/32 at 10 minutes, and so on.
This is with the worst-case assumption of instantaneous and complete mixing.
In humidity control, we know that although humidity is being expelled, it’s also being introduced by passengers. We could assume the same for the virus if all passengers are infected. New virus would be added along with new humidity. We know the humidity settles at a very low value in flight. And we know that not all passengers are infected. So the virus level would be even lower.
The point of this is not that virus transmission is rendered impossible, but is rendered unlikely by the constant dilution that is occurring. That discourages the necessary viral load for infection. In combination with masks, which further reduce the available load, this should keep the risk very low.
Ultimately the test of this is whether we see air travel clusters emerging. As of yet, we have not. You can argue that away as well, but as time goes on and air traffic builds, those arguments will have less weight. If we begin to see air clusters, then that would change the debate significantly.
Who checks that the HEPA filters are working. I can imagine bean-counters found a cheap low quality company or fake filters from China.
Also happened in the car industry, some exhaust filters were working at a rate of 1% for years because they were cheap.
Some airlines don’t even have all tools to check their systems. Some countries have low standards and low quality. Recently we talked about Boeing’s low quality too, they fired most of their quality staff, it was forbidden to find mistakes, unkown people signed quality protocols and the FAA wasn’t really interested to do their job. Who believes young Boeing planes are working 100%, I’m sure 6 months ago HEPA filters and the whole system wasn’t very important and very low on a safety check. No plane would have been grounded because of the HEPA system. Airbus might be better because I didn’t hear about such quality problems, but if an airline has low standards it won’t help.
Most important is many people are not careful and don’t wear their mask right, also hard to drink with a mask. And we see now what happens when fools are in power. Even Merkel didn’t wear a mask and had a stupid 1.5m excuse, later 3m distance was ordered when singing.
Expect the virus to spread. It should be done more to prevent it.
I want to protect my eyes, I still have googles from my freestyle swimming time. I will check if the glass gets foggy, otherwise will buy glasses against dust. Decades ago masks against radioactive fallout were fashion, sad I don’t have one.
Western Australia recorded 20 people infected with COVID-19 from one flight from Dubai.
https://www.abc.net.au/news/2020-07-18/wa-records-three-coronavirus-cases-dubai-flight-infections-rise/12469544
All the infected are all seated close together, pointing to mid-air infection event. Note that all international travellers arriving in Australia are quarantined in hotels for 14 days.
The authorities are investigating and doing contact tracing to establish whether the infection occurred in flight. Australia does a good job with this. In an earlier similar Emirates case in Hong Kong from June, with 26 people, it was established that the infections did not occur in flight.
This goes to the two issues I mentioned above, in flight infection transmission vs transport of infection. You could also have both simultaneously. Passengers have been arriving in Australia with COVID on a weekly basis. This event is a larger cluster on a single flight.
https://www.health.nsw.gov.au/Infectious/covid-19/Pages/flights.aspx
Think about this.
Objectivity and quality goes down the drain if a majority wants to stear towards an end goal, starts repeating each other, see what they want to see, inhales proof that supports the end goal. Any proof, indirect proof. Stubborns are ignored, overruled.
Ask Boeing.
If this turns out to be a cluster that occurred on the aircraft during flight, that will add weight to your arguments.
In July the number of scheduled flights worldwide has risen to 45% of 2019 levels, while passenger traffic has risen to somewhat under 30%. So that’s still some 60,000 flights per day, and some 3 to 4 million passengers per day.
If only 1% of those flights have a cluster event, that’s still some 600 per day. Or perhaps the time of exposure matters, so only longer flights carry the risk. Still we should be seeing significant numbers of reports.
You keep implying that I’m not objective, that Bjorn is not objective. Yet I am following the data closely, as I’m sure Bjorn is as well. He would not have written this series without substantial research and understanding.
For myself, if I take a position, I look for evidence of the opposing position, as well as my own. I could easily be wrong. If the evidence shows that I’m wrong, so be it. Being wrong is not a calamity if it moves you towards the truth. It’s only refusing to move that is the problem.