Leeham News and Analysis
There's more to real news than a news release.
Pontifications: No, it’s not time to fly
Aug. 10, 2020, © Leeham News: Frontier Airlines’ CEO Barry Biffle says “it’s time to fly,” reports The Points Guy.
By Scott Hamilton
Well, good luck with that.
Air fares are ridiculously cheap. Some airlines in the US continue to block middle seats and now require passengers to wear masks throughout the flight. Extra efforts are made to clean the airplanes. (Southwest Airlines, in a truly bizarre move, ceased cleaning seat belts and arm rests between flights—two things passengers are guaranteed to touch.)
Travel count in in the US is now up to about 800,000 passengers a day. This compares with nearly 3m a day pre-COVID.
I wrote July 6 why I won’t be flying any time soon. I wasn’t concerned about the airplane experience (except for those passengers who refused to wear masks). I was concerned about the experience getting to, from and at the airports and at hotels.
Now, there’s another reason why it’s not time to fly.
14-day quarantines
Long ago, The UK imposed 14-day quarantines on arriving passengers. Most of Europe banned US travelers entirely.
Within the US, some states and cities sporadically imposed quarantines on those arriving from highly infected states, whether by air, trains or cars. (Enforcement is questionable, but this is beside the point.)
New York City now has a 14-day quarantine on travelers from 34 states. As an island, checkpoints are easy to set up.
Chicago has a 14-day quarantine from 15 states. Enforcement is spotty at best.
With quarantines here and there, why fly as a visitor if you know there is a likelihood of having to isolate yourself (the UK, maybe New York) and a chance, however remote (Chicago)?
I planned to attend the Farnborough Air Show this year, as always. I bought my ticket, on American Airlines, in December (for the 2019 tax deduction). COVID reared its ugly head and FIA was canceled. Then the UK imposed a 14-day quarantine. I had a seven-day itinerary.
Flying made no sense.
(As an aside, when I contacted American about canceling the trip, the airline only wanted to give me the ability to use the ticket by December 2020. Fat chance for that. So I played a game of chicken. If American canceled the flights, by Department of Transportation rules, AA had to refund the fare. I waited, American canceled and I got my refund.)
My brother is in the Chicago suburbs. As much as I love him, I don’t want to spend 14 straight days with him. (His small condo is another issue, anyway.)
Experts say Americans are moving around too much right now.
So, Mr. Biffle, as much as I’d like to fly, it’s not time to fly by a long shot.
Comparing US deaths
The US now has more people who died from COVID than American military in World War I.
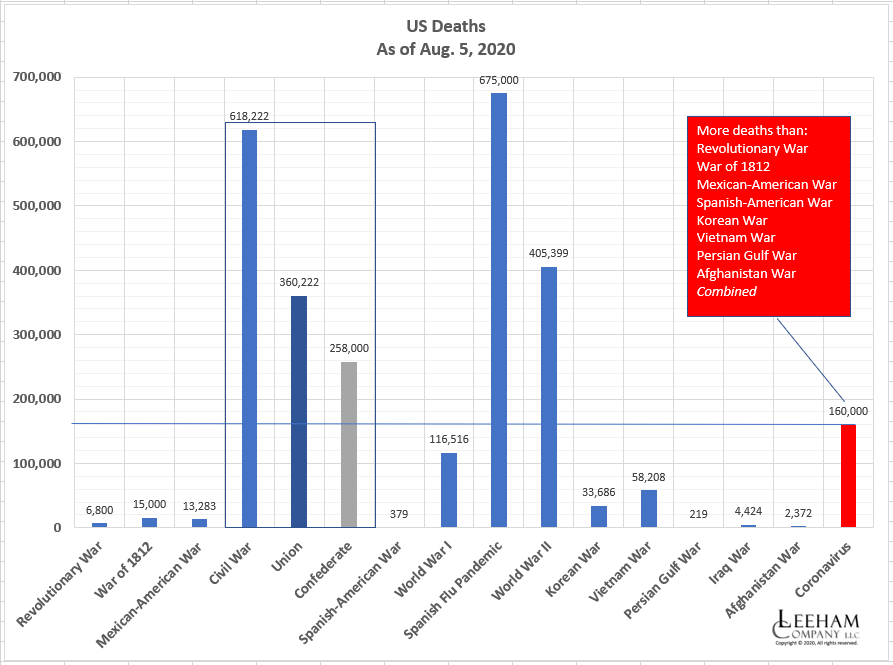
More US people now died from COVID than from the military in the Revolutionary War, War of 1812, Mexican-American War, Spanish-American War, Korean War, Vietnam War, Persian Gulf War and Afghan War combined.
Some models forecast there will be 230,000 American deaths by Nov. 3 (Election Day) and more than 300,000 by year end. The latter figure is more than the Confederate Army lost in the Civil War and approaching the Union losses in America’s deadliest conflict, ever.
For the life of me—literally—I do not understand how so many people in the US remain in denial about the risks presented by COVID.
Time to fly?
Not yet.
Your graph on American deaths for different events is truly enlightening and helps to put things in a more historical perspective. For one, that the first three wars that your nation fought were mere firecrackers in terms of deaths (I had no idea, thank you!). Secondly, a good argument against those that even today keep insisting that COVID-19 fatalities are not that many more than those of a bad influenza year (some are even as brazen as to say that in reality they are substituting one cause for the other, and that by the end of the year the total death toll for America in 2020 will remain largely unchanged).
I will take exception to so called mere fire crackers.
Each death impacts not just mothers and fathers, wives, daughters/sons or both, but all lives that person touched.
By your measure the UK was measly as well, though they were the only European power left standing by 1940.
WWI and II were pulling Europeans out of the conflicts they created thank you.
You should seriously rethink your cavalier attitude
Nobody questions the value of human life here. My remark was merely oriented at expressing my surprise at the very low (by today’s standards) death rate (in comparison to today’s conflict casualties, or even in comparison to contemporary European wars – Napoleonic Wars in comparison tallied 2.5-3.5 mln military, plus 0.75-3 mln civilians, for a grand total of 3.25-6.5 mln dead people). Or even in comparison to present American road deaths, some 38,000 per year, more than the first 3 American wars combined. No disrespect was intended was intended towards the deceased or diminishing the historical relevance of said conflicts.
Don’t worry, luisds: it was only TW who took exception to your post…and [edited]
I too was very surprised by the low death total for the revolutionary war. they never even mentioned numbers in all of the 8 times they taught us american history in school, but sure made it seem like there were a lot more than that.
I guess the reality is, you just can’t carry that many troops on square riggers.
apparently a total of about 50K british soldiers, and roughly 200k for the continental army (48k) and militias combined (~145k).. I guess with a 4:1 manpower advantage and control of local resources we should have won in a walk.
US had no arms or resources.
Spain was huge in supply Arms and Ammo, powder, France was second but also a big part.
Untrained troops going up against professional British troops totally negated the so called man power advantage.
Yorktown was due to the French Army (half the troops) and the French fleet.
Continental Army had meager funds and sometimes none at all.
It was a close run thing.
Normalize?
What was the population here?
Did tribal people support the revolution?
(In the War of 1812 with Britain, many supported the British because they saw worse treatment from the US.
Some say the US was lucky that Britain was drawn away by Napoleon again, as the US’ military was not competent.
Scott, speaking as an airline engineer in New Zealand who’s taken early retirement as a consequence of the effects of Covid, I think you’re absolutely right.
New Zealand has been in the fortunate position of being an island nation and, with an early hard shutdown driven by an empathic Prime Minister relying on the best scientific advice available, has worked as a “Team of 5 million” to eradicate Covid. The 22 cases extant are all amongst those in 14 day quarantine who’ve arrived from overseas. Within New Zealand, life is back to normal, without restrictions on gatherings or domestic mobility.
Yes, there’ll be economic fallout, but this has so far been cushioned to some degree by Kiwis holidaying in their own country instead of flying overseas.
From the outside, the approaches taken by some countries we have previously looked up to are utterly incomprehensible. The denial of many individuals is equally hard to understand.
Now is not the time to fly. New Zealand is only just talking about opening up a “travel bubble” with the Cook Islands, as they have no Covid cases. There had been talk of a similar bubble with Australia, but recent outbreaks there have seen this idea disappear.
However this may affect you all, I hope that you all keep well.
Thank you, a majority of us are doing our best.
Sadly an all to large minority could care less (I saw one person who lost two family members express the view that they did not think it was a big deal). You just can’t fix stupid.
“You can’t fix Stupid”, but Covid may cure it.
Good day Scott, very wise words indeed. This Virus is not going away anytime soon, and I am surprised to say the least at the flippant approach of the US Airlines to get as many people back flying regardless of the potential cost of lives.
Never let it be said that lives are more important than business.
Its not lives lost (think of the driver carnage) but what you can get away with (think Pinto with exploding fuel tank and its accompanying Firestone Exploding Radial)
As regards the 14-day quarantine-on-arrival:
Iceland and Germany offer inbound passengers the possibility to have a CoViD test on-arrival as an alternative to default mandatory quarantine. I think we’ll be seeing more countries doing that.
Emirates Airlines go a step further, and are now requiring all passengers to undergo a CoViD test max. 96 hours prior to departure…even for passengers who will only be transiting through Dubai.
As regards cumulative deaths from CoViD-19 in the USA:
Not wishing in any way to detract from the severity of the current problem, but there are other (non-infectious) conditions that kill far more Americans every single year, such as heart disease (650,000) and cancer (610,000).
Australia’s experience is that when people are left to their own devices,
about a quarter of people who are asked to quarantine at home are not at home when door knocked. I guess for countries accepting this reality, the COVID swab may be a palatable alternative.
For countries persuing elimination (New Zealand, Australia, China etc.) the only option has been to move to 14 days of supervised quarantine instead. This is because many arriving passengers would swab negative on arrival but are still incubating the virus and will only become PCR positive days later.
In Australia and New Zealand, the supervised quarantine regime incorporates two COVID swabs, at 3 days and ~10 days. This is combined with direct transfer from the international terminal via bus to a quarantine hotel where the guest will be required to stay in their hotel room for 14 days (under supervision of security personell).
And yet, as airtight as this procedure sounds, it was flagrantly violated by personnel at quarantine centers in Melbourne, which was one of the contributing factors to the present upsurge and associated lockdown in Victoria state.
I’m not sure how effective a policy of elimination will ever be. In the EU at present, it’s estimated that 30-40% of CoViD cases are completely asymptomatic, and similarly high percentages only demonstrate (very) mild symptoms that might easily be confused with hayfever. It’s probably present in every country, but not necessarily on the radar.
As the WHO keeps saying, CoViD-19 is probably here to stay, so there’ll have to come a point where people just start to get on with their lives and accept the risk. Remember that millions of people visit tropical countries every year, despite the prevalence there of diseases such as Dengue and MDR-malaria.
@Bryce: Vaccines will be the answer, one hopes.
Scott, I hope you’re right, but that may be wishful thinking.
Pharmaceutical manufacturers — and also the WHO / Dr. Fauci — are warning that vaccines may only provide short-term protection, and regular vaccination may become necessary. Somewhat similar to the situation with flu shots.
@Scott
As Bryce says vaccines are unlikely to be the definitive answer any more than they’ll help, as per flu vaccines
Readers point out that fatigue at following distancing mask and other measures is being felt all over the world, even in those countries normally understood as exceptional for their discipline
By which it may be seen that reversing the flow of industrial societies towards ever more intense socialisation and density can not be so easily reversed
Taking these two together, the possibility looms that the bug is here to stay for a long time, there’ll not be a great deal of relief from vaccines, which in any case will take a few years to appear, probably
Herd immunity as inevitable – part of that process is to come to terms with a higher mortality rate
Ironically NZ and other ‘successful’ at eradication countries will face a new dilemma – how to find/establish parity with the rest of the world, else be confined
All these decades of talk of globalisation, only to realise that this bug event is (real) globalisation, and the process is not as simple as had been thought- the more one isolates from diseases/nature, the more fragile one becomes
Your comparison with WWI is valid as long as it is accepted that the bug was created by misguided and failed human interventions – in the one case in the relations between nations, in the other in the relations between the practice of industrial agriculture and it’s locus in nature
Vaccines should help hugely.
In fascinating data coming out, T cells are emergent as a major factor (first line of defense which buys time to allows body to created specific Covd 19 anti bodies)
It turns out there are 4 cold Covd types out there. They found that some people are simply immune to Covd 19.
They think its a result of T cells getting Covd type programed into them as a intruder and deal with it.
Some also interesting aspects that recently getting a Pneumonia shot increases your response percentage wise by 28%
Having had a recent Polio vaccine does it by 40%.
Of course there are a significant minority that don’t think Science should be ignored. Its a shame we can’t remove what science has given them and get them out of the gene pool.
@Scott & Transworld
on vaccines please read this
https://www.lazard.com/perspective/global-healthcare-leaders-study-2020/
Understood, but vaccine will also get T cells programed.
As we are finding out, there is nothing simple about any of this.
@TransWorld
Little is known about this virus, even less about how to make and manufacture a vaccine and how effective it may be
Please read https://www.washingtonpost.com/health/2020/08/02/covid-vaccine/
@Scott – Vaccine may be or maglev may be
http://www.scmp.com/news/china/science/article/3096803/china-set-step-testing-countrys-fastest-ever-maglev-train-top
“Little is known about this virus, even less about how to make and manufacture a vaccine ”
There is an existing
Covid vaccine…for chickens.
There is a lot known about viruses in general , same with vaccines. Just finding the right pathway with those two will lead to a good result.
@dukeofurl
Re vaccines please read the two documents
Those in the vaccine industry report that finding and making to scale an effective vaccine will not be easy will not be tomorrow
https://www.lazard.com/perspective/global-healthcare-leaders-study-2020/
https://www.washingtonpost.com/health/2020/08/02/covid-vaccine/
Gerrard:
You are selective in what you are presenting. Yes I have seen that, I have also seen other information (such as the T cells).
You are ignoring or missing the fact that in parallel with the trails the vaccine makes are gearing up for production. If vaccine works, then they are ready to produce massive amounts.
Yes, if it does not or the Virus morphs like flue, its partially wasted or possibly all wasted. Wasted money is the risk vs the clear possible gain.
Clearly what is emergent is the Covd type cold virus has provided a T cell program.
While anti bodies fade off, T cell programing stays.
This is also a different era with more knowledge, resource and computer modeling as well as recent advances in the art of vaccines including SARs and MERs research.
You can crunch massive amounts of data now we could not before. Ergo, they can see a recent Pneumonia shot has a major affect in immunity.
A WWII Sherman tank is nothing like an M1 Abrams.
Using a Sherman tank as you base of understanding of modern armor would be just as wrong as using the past vaccine operations as your basis of understanding.
When the background data changes your understanding either changes or you are going to be wrong.
@Scott – Sorry to add to vaccine reports, but here is one that casts new light on how a vaccine may/will not work for those most in need because most vulnerable- the obese – by this count 42% of US population
khn.org/news/americas-obesity-epidemic-threatens-effectiveness-of-any-covid-vaccine/
@Transworld
The two reports are contemporary and deal with the views of vaccine makers in the Lazard survey, and more generally with those of ‘experts’ in the Washington Post article
Neither are discussing the past – and if they draw conclusions based partially on experience this can only be regarded as and integral part of any scientific enquiry and manufacturing venture
Both articles are as comprehensive as representative – I do not select them as two among many others which give diametrically different opinions/results
Generally the experts and the industry are very cautious about vaccine prospects and success
Read the third report posted which suggests that a very large minority, 42%, of the US population will not, in the event of an effective vaccine, draw benefit
@ Gerrard White
You’re wasting your time: you can drag a mule to the water trough, but you can’t force him to drink.
Some people don’t make a distinction between fantasy and realistic expectation. They also try to scapegoat, by electing an imagined culprit. And they throw a tantrum when confronted with a contrarian opinion, because it erodes their sense of certainty and self-ordained expertise.
Crises like the present one provide a fascinating window on the human psyche.
@Bryce
It appears as if many people wish to think right and do right in face of the bug – which means adopting for themselves a simulation of low density living with polite and precise, even objective, adoption of cleanly habits
This well regulated responsible life style they would like to see commonly adopted, and are convinced that this well behaving and well meaning attitude is the solution
This is a technocratic mind set, it is to place considerable faith in ‘experts’ and in ‘technology’ – which involves an avowed conviction that one or more vaccines will be invented, will scale, and will be sufficiently successful to require only the maintenance of the other measures to ensure and procure long term success – world wide
Apart from any other consideration as to the realism of such an attitude one may note that it bypasses or feigns to ignore the often stated recent opinions of most WHO spokesmen, and other ‘health experts’, in particular leaders of the pharmaceutical companies (all members of the technocracy) all of which indicate that the vaccine, if ever ‘invented’ will be no more effective than a flu vaccine, perhaps less so, will be hell to scale, will not be coming anytime that soon, even if dating this they are as cautious as in that estimate of effectiveness
The paradox – faith in technology gave rise to this bug in one division of modern technocracy, ind ag ; yet other members of this same technocracy can not fail to be over optimistic that the technocracy has the technology to provide the solution, provided we all go along with their dictums show real discipline and behave to plan
But – take away the vaccine….and what’s left ? Nothing much – low density living in industrial societies is the reserve of the rich minority : so they hope for a vaccine, meanwhile we are all to behave properly and join in the chorus of hoping
Scott, waiting for vaccine that is safe enough is a fool’s game, you can’t predict how soon. (Wanna sign up for an MMA? 😉
Achieving herd immunity is a way, and it may be sooner than thought given the number of people who were infected but not reported, and the possibility that some people are immune for other reasons such as having antibodies for a different corona virus like SARS v1 and possibly some strains of INFLUENZA (the perennial killer) and even the common cold.
Recognize that SARS-CoV-2 is not a great risk for most people, the essential is shielding the vulnerable. Florida did that aggressively, Sweden eventually did that – without significant lockdown. Care residences and hospitals are where at risk populations are, by definition most people in care residences are in quite poor health. As with INFLUENZA, lung deficiency and heart deficiency are the big risk (heart essential to good lung function). Poor body function due to other things is also a risk, such as kidney and liver problems.
Yet most governments failed to protect people in care residences (aka nursing homes). And failed to prepare for the inevitability of another pandemic – did not have plans in place, did not have anywhere near sufficient PPE. Fortunately an entrepreneur in South Korea switched his company to developing and producing a test for COVID-19 infection, and companies in Canada and the US – plus schools and hospitals and clubs – jumped up to make PPE and disinfectants. (Booze makers became useful by using their alcohol to make hand sanitizer gel.) A small example of having a good plan was Florida, which jumped into care residences that were already on a list as marginal performers, then worked with the better ones. In contrast, B.C. had severe problems because care aides were working in more than one facility so cross-infected, then was slow at stopping that (whereas a private residence with some customers receiving government service replaced government aides with private nursing, within 24 hours, he’ll get good business).
True but … It is apples and oranges comparison. The other deaths do not cause economic collapse and a great depression.
Very useful and timely information on flying. Thanks Scott.
CoViD-19 isn’t causing “economic collapse and a great depression”.
It’s the current response to it that’s (at risk of) causing these things.
Most people who get CoViD recover from it in a few weeks, and get on with their lives.
Some people who get CoViD have a much longer recovery trajectory. But we already have MANY people in society with chronic conditions (diabetes, COPD, IBD), and we still chug along just fine.
It’s very unfortunate that CoViD also causes fatalities….but, as pointed out above, there are other “everyday” conditions that cause far greater numbers of fatalities.
Summarizing: we’d all do well to adopt the mantra propagated by the British during WWII, i.e. “Keep Calm and Carry On”.
@Kant
Well they all use military metaphors and language to talk about the bug – lockdown, battle etc etc
In the minds of the folk they are at war- although probably this is a deliberate illusion fostered by governments to attempt to make everyone into soldiers of their own fortune
If your nation is on the losing side in a major war then you do suffer economic collapse, generally speaking
Bryce:
Clearly you do not get it nor want to.
Those deaths are added not subtracted from all deaths.
And those Covd deaths mean someone is in ICU for a period of time taking up and exceeding what is normal excess capacity for the normal ups and downs.
You can add in other health care disruptions (how many die because they could not get treatment for separate from Covd?)
You also have not a clue what the long term health impacts on those who recover but have damaged hearts, lungs and other systems. Clearly you do not work in a science driven world.
Models can only suggest, but 3 million possible deaths if we do nothign is incredible impact and can indeed take a society to its knees.
UK Deaths in WWI were a huge economic disruptive factor post WWI. Which then failed to be armed in 1935 which in turn was part of Hitlers calculus going into WWII.
Frankly if you want to do yourself in that is your choice, its not your choice to inflict your demise on the rest of society.
Your rights stop at the end of your nose and they don’t extend into the rest of ours.
Its your type attitude that got us this deep into this disaster.
You need in the graph the motor vehicle accidents 36,560 and gun homicides 11,004 = 47,564 and this happens every year.
Look at the hospital caused deaths each year.
I believe its around 250,000 in the US.
There is a relative aspect (sadly). Its a steady number the the system has grown up to deal with, not a inflationary spiral like a pandemic.
And this is one I’ve argued with my medical wife for many years. Her response is that:
– it’s not an apples with apples comparison, since people do not come off a production line i.e. we’re not identical
– people may have underlying conditions which they’re not aware of, some of which may be significant, others not
– people coming into hospital are typically more scared than those coming to an airport, yet they still want to have their operation over and done with. This can lead to concealment of some elements of their condition
– some interventions e.g. in the heart or brain, can be likened to low level aerobatics in that if it goes bad it can do so suddenly and quickly.
There are also cultural, regulatory and other differences between aviation and medicine, amongst them:
– the fear of litigation (New Zealand has avoided this by introducing a system called Accident Compensation; avoiding litigation but not scrutiny of medical misadventure)
– lack of mandatory reporting
– no mandatory equivalent of safety management systems (SMS). My wife reported one surgeon’s rejection of checklists on the basis that “I’m not going to have a nurse telling me what to do!”
There is a gradual adoption of some aviation practices in medicine, but it’s slow. This is not to say that there aren’t things aviation could learn from medicine, by the way.
Agreed for the most part.
Interesting on NZ methods and clearly we need that here.
Medicos tried to kill my brother twice. Not due to his condition but infecting him.
There are two types of IV. One is short term, one is long term.
First time they did use a short term IV for a week and gave him staff.
then they tried to do it again (he was astute enough to nail them but I was a half a micro second behind him) .
The difference in IV type and how not to use a short term IV is as basic as breathing and they did it anyone. Stupidity and incompetence of it is stunning.
Equally as clearly it was not a one off.
Hence the value of checklists and a QRH handbook equivalent. Some of the medical profession is trying really hard on this.
Interesting historic comparison, I agree.
Statistics like this help you objectively rethink forces behind big events like the cold war, Israel’s position and more in general: traumatized populations acting “unreasonable” for a few generations, from our western high ground perspectives.
Civil wars are the worst, if you ignore the huge wars of destruction in Russia and China. https://upload.wikimedia.org/wikipedia/en/b/b7/Deaths-of-WW2.gif
You make a good point. Ironically I am now traveling for a job interview this week and had to plan around these restrictions. With the other violence in Chicago, NYC etc I don’t know how many would want to go there anyways right now. The other issue is if you contract Covid while there. In this trips case, I could drive 9 hours home, but what if it was the other side of the country?
As I mentioned on an earlier report, they may have to design aircraft with contagion in mind. Obviously, with fewer seats… Per the reference to the A320, max capacity 150. Also, you could drive to see your brother…
@Sam: Of course, one can drive just about anywhere. In my case, it would be a four day drive.
On a related note:
Before CoViD came along, the Flight Shaming fad in the EU was causing some foreign exchange students to shun flying from Europe to China and to take the train instead. The result was a journey that took 14 days instead of 12 hours, as well as being MUCH more expensive. Ironically, it also caused a much greater environmental footprint that flying.
@scott – 2 days max. I drove from Boston to Vancouver in 3.5 days in late december through blizzards and ice storms from Minneapolis through to Spokane. first night in south bend indiana, second night in Bismarck ND, third night in Coeur d’Alene Id (weather got really bad around Butte Mt, slowing travel down to about 30 mph from there to Coeur D’Alene) and at Vancouver by noon.
Chicago is easily 2 days this time of year…. you just have to want it 🙂
@Billbo: Google maps says 30 hours from Seattle to the Chicago suburb where he lives. Maybe you can drive that in two days, but I’m too old to push myself that hard. Three days feasible.
@scott – I am a bit of a psychopath on long drives, 14 hr days the norm and no stops longer than a potty break… my wife’s family is from North Dakota, and for me that is a 2 day drive from Boston. my wife will take 4 or 5 for the same drive.
More power to you, billbo. This old body can’t do that.
Uh, ‘bilbo’, two days is a push, be safe. 12 hours driving when younger than Scott and I is much, yes I did Vancouver BC to Calgary in one stretch a few decades ago, IIRC about 700 miles. Monitor yourself, perhaps take naps, stretch, and stay hydrated.
Unfortunately not many museums and such will be open along I-80. There’s an AF museum not a long way north of I-80, perhaps ‘Castle’, that has a large aircraft like a B-36 or XB-70, the other of those two being in OH IIRC. (Of course Scott has a good museum at Boeing Field.) Take time, do work from motel rooms.
(Even in summer from the Puget Sound area I’d take I-90 through the Cascades then angle down through Yakima to the tri-cities, over a bridge, up onto the Baker Plateau I call it, picking up I-80 just east of (big city north of SLC), straight on to Chicago.
Sam:
No one is going to design aircraft capacity based on in a hundred year event.
And yes I pulled the once in 100 years out of my ear, based purely on 1918 Pandemic.
That makes sense, but two buts come to mind: 1. They can exchange the air faster; 2. Because of global travel contagious diseases are on the rise.
Sam:
They can are doing a lot (or in some cases being stupid)
You don’t have to desing change anyting, just a governbemtn mandate on searing distances and no isuse.
Bjron has covered that, it seems pretty good on the plane.
I thank him, as it was his information that allowed us to get it to work when things got dire.
So far, the two family members that traveled have tested negative on arrival , one week in and the one going back gets tested this week.
Actually the best test is one week in (while isolated) as you have it then or you don’t.
A negative now just tells you that you didn’t have it a week ago, not that you just caught it in the last few days.
CoViD fatigue is starting to become rampant here in the EU: whether it can be rationally justified or not, more and more people are getting lax in their adherence to CoViD rules, such as social distancing.
Even in ultra-disciplined Japan, CoViD fatigue is now becoming evident in Tokyo.
I think that more and more people are going to realize that they can’t continue to postpone their lives, and will re-commence flying relatively soon. The only factor that’s holding me back at the moment is the 14-day quarantine rule — apart from that, I’d get on a longhaul flight in the morning without hesitation.
You might not hesitate, but many other people would.
I will not be flying to visit my elderly parents at the current risk levels. And, as for work travel, our company is not allowing business travel at the moment.
We did have two family members fly. It was a crisis situation.
Voluntary? NO way
We live in California and like Scott’s brother, my parents live in a Chicago suburb (actually literally across the street from Chicago).
Given the current situation (2 young kids, elderly parents (dad is a diabetic), people not following protocol, no vaccines etc.) we’ve decided to hold on ANY travels this year – or until a vaccine is available.
I know my parents are old and they would love to see their grand-kids this year (we go to Chicago every year actually), but not taking any risks is the best choice IMHO.
Of course, everyone’s situation is different however I believe many people/families are in the same situation as we are.
The other side of that coin is that you’re implicitly assuming that your parents will still be alive and well when you start traveling again…when, of course, one or both of them could die in the morning (e.g. from a heart attack). You need to be careful when weighing possibilities against one another.
A lot of seniors are starting to adopt an attitude of “Heck, I’ll take the risk…I want to see my family”.
I have had a good and wonderful relationship with my mother for 60+ years
If she dies before I can see her, I will miss her terribly but putting us both at risk for a visit?
If you have to rush to visit family then you have lived your life badly and it will not fix that.
So the response is valid for that person. What you do of course is your choice. I just hope you don’t impact others.
Of course, life is full of risks and choices however one has to evaluate the bigger risk.
Fortunately my parents are healthy overall so we’ve taken the decision that waiting until a vaccine is out is the better (risk) outcome.
Maybe by next year if we don’t see a vaccine we might decide to take a multi-day road trip each way. If and when that time comes, we’ll figure it out.
With the lack of activity in the world of manufacturers, suppliers, and users of aircraft, I hope Leeham News and Analysis can continue to flourish, especially with the increased number of contributors. I wish you all the best even as we lack excitement in the industry. Maybe you can branch into commentary on space, where there is continuing activity and innovation ! Maybe we will have a few commercial travelers in the near future !
It helps to view the death statistics in terms of excess deaths (more than would normally occur).
COVID has an excess death rate of about 12% in the US for 2020 through July. There was a large peak early on, the excess rate in July was about 6%. It had dropped to almost 3% in early June. These figures are above the normal death rate, which varies seasonally but is around 50K to 60K per week in the US.
For the Civil War period (4 years), the excess rate was around 125%. For the WWII period (4 years), about 8% within the US alone.
The virus infection rate can be managed by good practices. Especially important to protect those who are vulnerable, since deaths are concentrated there. And to realize that the virus will resurge if given an opportunity.
Within that framework, many activities can resume, but some cannot, and some must resume differently. This will be true until a vaccine is available, and probably for some time after until the effectiveness and duration are better understood.
So I think it’s about understanding of risk and smart use of activities, rather than blanket statements endorsing one side or the other. The more we do things smartly and restrain the spread, the more activities will be possible, and the economic damage will be reduced. The less we do things smartly, the more restricted we will become, and the more damage will be done.
New Zealand is a good example of this. Within the country, many activities and the local economy can resume.
In my area, schools are being hotly debated now. It’s difficult with kids to manage their interactions. So it’s looking like some parents will opt for in-classroom and some will opt for at-home learning.
If we had done better at reducing the spread, this would be a more certain decision. But as things stand, there is a lot of uncertainty, we won’t know until we see what develops as schools reopen.
One problem is that in my area, most people only are aware of a few others that have had COVID, and were quarantined. So the personal experience doesn’t match the news, until after it’s too late. So when some leaders and commentators say it’s not that bad, that message resonates, even though it’s a simplistic view.
The issue is that some people are simply stupid and impact the rest of us.
That includes leadership on down.
As we are stuck with stupid people, good leadership is the only answer and we do not have that (none at the national level).
NZ can control the lanes, as a nation of 350 million or so, we cannot.
Side by side states can have two totally different response and infection comes in from outside.
While the so called National response was to stop China travel, that was not the reason. They left Europe and Latin America travel untouched.
New York in turn was infected from Europe not China or Asia.
We are stuck with what we have Nationally by less than majority due to a legacy of the Constitution that should have been abolished with Slavery (or before fore the sake of both)
NZ is fortunate in its isolation and leadership.
In the US until this is handled, any gathering is a major risk. Restaurants and bars have proven to be two huge ones, probably the next is stupid outdoors and indoors gatherings.
There is no mechanism to locking up the idiots and letting Covd run its course with them.
It’s more than just individual stupidity. Many people aren’t sure what to think, and so look to others for perspective. On some talk radio and news channels, there is a 24/7 attack on the medical professionals at CDC, NHS, and presidential advisors.
The given view is that local medical professionals, doctors and nurses and healthcare providers, are doing a great job. But the policy makers who guide them, have seriously botched the whole thing.
If you talk to the local professionals, they endorse the guidance they’ve been given. So that narrative is not truthful, but it has political value.
For people who aren’t able to judge for themselves, those argument carry weight as they are asserted with absolute assurance, and they offer an explanation of the outcome we’ve seen. And so we have not had the response in the US that we should have seen, because there is not agreement on the science or the facts. Those have been overtaken by largely political views with other agendas.
It’s an extension of the general dysfunction we see in leadership, and for the same reasons.
@Rob
There is an old saying – Countries get the leaders they deserve
‘If the people are unhappy with their government, they should know what to do’ Abraham Lincoln
Rob:
People that can’t judge for themselves?
So what you are saying is those people also should not be allowed to vote? Drive cars? Have children?
No, its people who refuse to educate themselves. They are the same ones that flock to restaurant that are open illegally (or go to political rallies and chant)
Some of the smartest most capable people I met did not graduate from high school.
Either they are adults and make themselves capable or they revel in the ignorance and like to stay that way.
Unfortunately they can also drag the rest of us down with them. So no, they do not get a pass.
TW, your response proves my point and is an example of the issue at hand. Your view is that other people are stupid and you’re not. Trouble is, those other people are saying the exact same thing about you.
Ultimately the public discourse has to be truthful and open, with respect for knowledge and evidence and those with expertise most people may not possess. It’s not necessary (or even possible) for everyone to be an expert, if the experts have traction in the discussion.
If instead they are met with resentment or disdain by people who believe they know better, then the outcome won’t be good.
Adding to the countries already mentioned above — Iceland, Germany and the UAE — Greece has now also announced that all travelers entering the country will need to present a negative CoViD test result less than 72 hours old. Tour operators / charter airlines are directing passengers to labs that will perform the test for a nominal fee, and — in many cases — this fee is being absorbed by the tour operator / charter airline itself.
So, it looks like this may be becoming a new norm.
For those pinning all their hopes on a vaccine, articles like the following are very informative:
https://www.theguardian.com/world/2020/may/22/why-we-might-not-get-a-coronavirus-vaccine
As it happens, Russia announced today that it’s going to start rolling out a vaccine, although phase 3 clinical trials have not yet been completed. It will be very interesting to see how that pans out.
Breaking news from the Antipodes: New Zealand is back in partial lockdown after 4 cases from one household were found today. Presently no idea how this has come about – this virus is a challenge.
It was probably there all the time…unnoticed, under the surface.
As I said in a comment above: 40% of cases here in Europe are completely asymptomatic, and a large portion of the remainder involve symptoms so mild that they could easily be dismissed as hayfever. NZ is deluding itself on this point.
I don’t think NZ id deluding itself, they are trying to walk the beam and the bias is to fall off on the side of normal.
Smart is when you move the beam over as you find out what you can and can’t do.
NZ is unique in its isolation and can operate differently that the US , Europe etc.
China is effective as well as they do a massive clamp down when it pops up. Not something a Democracy can do.
Seems like it might be able to hide out for longer than 2 weeks. If mold spores or hantavirus can be latent for months or years, maybe 2 weeks is wishful thinking.
Reporting now is the virus may have come into New Zealand on refrigerated freight. An infected person worked for an international refrigerated storage company. The virus can be dormant and then reactivated in cold temperatures.
This would make sense as the vector if proven to be true. Then there’d need to be additional precautions when handling the freight,
Bottom line is that resurgence is always possible, so good practices have continuing importance.
Yes, we’re immediately in hard lockdown here, broadly accepted as a necessary evil.
The problem is that so little is known about this virus that it is hard to identify good practices.
I’ll keep you all posted; for the moment, people are working from home and all shops – supermarkets and petrol stations excepted – are closed.
The lockdown will be brief unless a wider dispersion is found. Remainder of the week at present.
The important thing in New Zealand is they have a plan prepared and ready to go. By acting quickly they can limit the impact and regain control, thus having a quicker resumption of activities. The time scale of their response is appropriate for the virus.
@Gerard
Reports of panick buying in the press and photographs of crowds running amok
Can NZ afford to lockdown at every appearance of the virus? And for how long?
Not only the length of each lockdown but for how many years into the future do the authorities project that this measure will be used?
Until replaced by…?
Has anyone any idea of how to measure the impact of lockdown and quarantine not only to economic and social life but in terms of health?
Is such a measure being used in NZ to assess virus response?
@Gerrard White
Although I understand (and subscribe to) your points very well, a small distinction that deserves to be highlighted in this case is that it’s a CONTAINMENT lockdown (like the recent events in DaNang in Vietnam) rather than a MITIGATION lockdown (like the one in Europe in March/April/May). Strictly speaking, a containment lockdown can be relatively short (10-14 days) and highly localized.
As regards mitigation lockdowns, many countries in Europe now have an attitude of “never again”. The current trend seems to be that, if relatively simple measures like social distancing, face coverings, proper ventilation and widespread testing don’t adequately control the virus, then it will just have to run its course.
As regards your penultimate point: in the country where I live, a second national virus management team has been formed, which predominantly comprises experts in sociology, psychology, logistics and economics…as opposed to the first national virus management team, which only comprised virologists. That really says a lot!
Gerrard White, people in New Zealand haven’t “run amuk” due to a 3-day closure in one city, so that testing can be performed and the potential virus cluster evaluated and interdicted.
Like everyone else, New Zealand is learning as they go. This is the first recurrence in 100 days. They will adjust their response based on what is learned in this instance, and continuously improve over time. But unlike most of the world, they are starting from an excellent baseline.
You constantly seek to belittle their achievement, but there is no arguing with their success. They’ve done a great job by erring on the side of speed and containment, which now allows them the freedom to loosen as they feel is safe and warranted.
What is the economic damage of erring on the opposite side, or not doing enough? You don’t have to look very far in the world to see.
The effective transmission rate in the US was extremely high as the crisis began. Now, even with the uncoordinated response, it is down around 1.0 for most states. It took too long and some gains were lost in the last few months, and had to be regained. But there has been improvement over time.
Much of the world has done better than the US. All areas have seen some degree of resurgence, but not to the extent of the original outbreak. New Zealand was extremely effective in attaining that improvement, in much less time than elsewhere. There is something of value to be learned from that.
@Rob
Look at the videos of the supermarket scuffles, a very middle class amok to be sure
The NZ and Aus severe lockdown was doomed from the start – the bug is produced by one of the technologies of globalisation, the bug is global, and will only be dealt with globally, one or two countries may protect themselves initially, but will not be able to isolate from the rest of the world for long– certainly not for ever
Such attempts are foolish and misguided in the sense that false hope is given by the initial success of martial laws – & fulsome world wide congratulations – so are then very difficult to renounce
As for the vaccine…well…..
@Bryce
I take your point about the distinctions in the intended results for the lockdowns, at least the stated intentions
Nonetheless it might seem inevitable that flare ups as currrently in NZ and Aus to mention only those may continue for some while, perhaps some years
Has the math been done on the costs of these lockdowns, social health and economic – or is there no alternative considered to lockdowns, thought to be no point in doing the math ? Government policies instituted without such would not appear well founded
The point is considerable –
Countries like NZ and Aus eliminated at first the virus, only to suffer ‘second waves’ presumbly originating from outside (but perhaps not, maybe) – if a second surely a third is possible/probable, and so on
The rest of the world is considerably infected, the bug can travel in on one person, in food, perhaps in animals ( ?)
Therefore -To quarantine even a very great deal less than the pre virus number of travelers will still leave open many possibilities/probabilities for transmission, to a population weakened as far as resistance/immunisation by isolation, and by martial law, not the best way to bring up a family
You say that in Europe they have realised lockdowns are not going to work, and they will let the virus run it’s course – perhaps they will or have taken an attitude similar to that in Sweden – but I guess they still wish to quarantine ( ?)
The Aus and the NZ got off on the wrong foot, thought they could isolate at a national level from a global event, for which mistake both countries will now start to pay the price
I read reports from India which state that the slums of Mumbai have reached herd immunity – and with surprisingly low mortality : they did this without masks, without social distancing, without hospitals, without…. anything except tough good health determination and courage, and because they could not play around with lockdowns or quarantines or any other maneuvers which put off the inevitable for a week or a month or two and offer the fake comfort of false illusions
Gerrard White, the evidence is against your position. Countries are making progress in reducing the transmission rate, and that will continue with or without a vaccine. It’s likely a vaccine will have at least some benefit, and contribute to general resistance.
It probably won’t be possible to reduce the transmission rate to zero, so in that sense we will have to deal with the virus for the foreseeable future. But it can be managed with proper precautions and adaptation of behavior.
New Zealand points the way, as they have managed things really well. Their exact methods may not work everywhere, and some adaptation may be needed. But to say that their efforts are pointless is to say that failure is preferred. You may believe that but the vast consensus of opinion is that success is the better option.
Also to answer a few more points:
1. The panic buying in New Zealand was a public over-reaction, but not indicative of problems in their strategy. Stores have reassured the public that there are no shortages. They were to remain open, but with fewer hours and less patrons at one time. The same thing happens here when a blizzard is forecast. People empty the shelves of supplies out of anxiety (just in case).
2. The slums in Mumbai have only about 5% of the population over age 50, which is the vulnerable group for COVID. This is because their life expectancy is under 60, which is in itself a tragedy. 50% are under age 15, 75% under age 30. So it’s possible to have large rates of infection there without as many deaths. Contrast that to 33% over 50 in many developed nations. The outcome and cost of unrestricted infection would be very different.
I don’t think we should hold up that circumstance as the example to follow. I’d rather hold up New Zealand as a better and more desirable outcome.
Panic buying only lasted a day in NZ supermarkets quickly shifted to limits on the the usual items . Reports are now that its quickly back to the situation that was happening near the end of the previous lockdown.
@ Rob
The Mumbai slums are not held up by anyone as an example of ‘success’ but as an example of the reality of the world in which a large percentage of the population lives in these or close to these conditions
In this case it seems that they have been quickly through the worst of the viral infection – when other communities richer and more prepared to buy time are now facing the worst : ‘experts’ expect this northern winter to be worse
As a very large number of people lives beyond the reach of all the nostrums of masks distancing lock downs and vaccines, in every continent, then all these measures are to no avail in a global ‘cessation of transmission’ or elimination sense
Hence the misguided and foolish nationalistic policies of Aus and NZ – these places are too small and too dependent to isolate and survive – any attempts to do so
will fail and they will have to, one day, modify their measures accordingly
Such narrow minded nationalism is indeed ridiculous and outdated in the face of a global event
The fact that these and other countries, or their governments, failed to take any measures in common in co operation and collaboration with others, is the world wide failure to understand how to deal with a world wide phenomenon – easy to wreak global damage impossible to repair
Nothing ‘of value’ comes from initial success if it is only achieved at the expense of long term failure, if it is achieved by misunderstanding the nature of the virus, and if it severely damages not only democracy, health, society, economy, and the possibility of correctly using ingenuity and resources to handle a common danger
This is what the ancients called a Pyrrhic victory
You in America are very lucky you have been so inefficient and so in capable and so dis organised as to fail in your attempts to behave like the NZ and like the Aus – you have found that you have more in common with and more to learn from the poor in Mumbai than the rich in the South
A bitter pill? Not at all – the new normal
Gerrard, your basic position is that we should yield to the virus, as the situation is hopeless anyway. Accept that advances in knowledge and medicine in the last 100 years leave us no more able to respond than then.
That view is wholly irrational. Let’s look at it first from the human perspective:
The endgame and only way forward is to develop resistance in the population, such that illness and death from the virus are minimized in the long term. So what are the ways for that to happen, what is the duration of that protection, and what is the cost?
In the example of Mumbai, which is closest to your ideal, lack of resources and inability to isolate or distance have given the virus free reign, in a population with only a small segment vulnerable to death. This will likely establish biological resistance, at the cost of extensive illness and a limited number of deaths. There has been little economic cost because there is not an organized economy. The biological protection duration will be at least 6 to 8 months, probably a year or more. The need for vigilance is greatly reduced, and indeed no options may be available anyway.
In the example of Sweden, resources were brought to bear to limit rate and impact, but a deliberate decision was made to allow the virus to propagate in the population. The results have been mixed, there is not yet general biological resistance, although the use of resources has induced an artificial resistance in reducing the rate of spread. The protection duration for the biological component is similar to Mumbai. The artificial component has no duration, it must be sustained by the continued use of resources. The cost has been a moderate reduction in economic activity, as well as significant illness and deaths in the vulnerable population. Moderate vigilance will be needed until the biological resistance becomes dominant.
In the example of New Zealand, the emphasis has been on the use of resources and restrictions to induce artificial resistance, with the goal of halting the spread. There is no appreciable biological resistance, but also no appreciable illness or death. The artificial resistance must be sustained by continued resources and restrictions . The cost has been brief periods with no appreciable economic activity, followed by reopening again with far lesser activity. But the need for vigilance is constant and the inevitable flares must be addressed by continued partial restrictions.
All of this has taken place without a vaccine. If and when an effective vaccine becomes available, the impact will vary by scenario. For Mumbai, a vaccine will be beneficial but will not have substantially altered the trajectory of the virus. For Sweden, a vaccine will accelerate biological resistance and significantly reduce further illness and death. For New Zealand, a vaccine will introduce biological resistance and greatly reduce the need for continued resources and restrictions. It will not appreciably reduce illness and death because those have not occurred, but will allow full economic activity to resume.
So looking at these societal alternatives, which is preferred? I think most people would choose the New Zealand scenario if they could. Obviously most of us can’t choose, but our leadership could over time.
Now let’s look at it from the perspective of the virus:
The Mumbai scenario is ideal, in that a large & young host population is available, with fewer production losses due to deaths in the aged vulnerable population. The large number of hosts increases the odds of mutation that could allow multiple passes through the population. If multiple waves can be developed, a scenario like Mumbai offers the best opportunity.
The Sweden scenario is mixed, the rate of production is slowed as the potential hosts cannot be utilized as quickly or effectively, and a larger vulnerable population means greater production losses. But inroads remain possible, and are improved if the human guard is let down. Opportunities for multiple waves are diminished.
The New Zealand scenario is a disaster, no appreciable foothold can be attained in the host population, so little or no production, and apart from sporadic and brief flares, the environment is not survivable in the long term.
So again, which of these scenarios is preferred? I suspect most people would rationally choose New Zealand.
As far as the disparity in development and resources between areas of the world, that continues to be a problem. One can hope that once the developed nations finish competing for initial vaccine production, that capacity will be turned toward the rest of the world. The Gates foundation is focusing on that, they’ve been trying to deploy vaccines worldwide for a long time.
@Rob
You make many incorrect assumptions, always a no no when in debate
‘Your basic position is that we should yield to the virus’ – nowhere do I state that : I say a vaccine is perhaps dubious in effectiveness accord to the Pharma industry, and I say hand washing masks distancing are the reserve of the rich
To yield to the virus -what can that mean ? – to command oneself and one’s immune system to not resist infection ?
This appears to be impossible, to be masterful to such a degree so to oppose body and nature – but perhaps the technology exists ?
However most of the world has to be realistic – as the poor in Mumbai : this is not claimed as an ‘ideal’, given there is none, there is just more efficient survival – what I say is that it appears herd immunity has been achieved fastest there at not over considerable cost of lives or labour
I say you in particular (your class, your mind set) are misguided, and you do not pay attention to the experts and the industry, and in particular as well countries like NZ and Aus are foolish and mistaken and making an attempt at authoritarian measures of which they have little experience and less command and for which no long term patience
You concentrate, at the expense of reason, at the expense of an understanding of viruses and the general nature of human health, at the expense of logic, on those symptoms you see as manifest, and you wish to treat those, but not the cause
This virus was manufactured by human agency, ind ag, and may, with difficulty, but may be restrained in the future by human agency – industrial agriculture may be restrained or constrained or modified
Please research ind ag and the production of such and similar viruses – that is if you are not aware of this causation
Then you will observe the means of production and will be able to think about a solution, to what may it resemble, how may it be achieved
Until then all you are doing is running from one band aid to another, only to glimpse a virus which is not only quicker, elusive, better at logistics, and – in a word – more intelligent, you are always playing catch up with something that has already won, just like Achilles in the story
It is possible to live with this virus without such large amounts of self inflicted damage as seen hitherto, it is possible to palliate the disease, it is possible to upgrade one’s and one’s community’s health, it is possible to so modify the conditions of production that the virus will cease to mutate over from bats and so forth into humans
Perhaps you have never been to NZ, perhaps you have, but you should know of what you speak when you say most people would prefer the NZ solution : I would not like to disappoint you but NZ recent history might tend to show they will not be able nor willing to welcome immigrants for quite some time, and given how few of them they are on those really quite large well placed and fertile islands it appears possible to conclude that either they have always felt that way, or else the rest of the world has, or both – it’s probably easier to isolate if that’s all you have ever known and ever will
If, on the other hand, you wish to change the nature of politics in your own country to more closely resemble NZ, you have only to collaborate and convince a majority at the moment hell bent on very much the opposite, but read Abraham Lincoln for the how to
The claim of industrial agriculture as causation is not valid in this case. The virus emerged from natural interaction between species (bat and pangolin), followed by human interaction with the pangolin in the wild, via illegal poaching and trafficking in animal parts & meat. Pangolins are not domesticated or farmed.
The remainder is a dissembling descent into socio-political beliefs, which I cannot follow. I don’t know what COVID has to do with Abraham Lincoln, or immigration policy in New Zealand.
So I’ll just stand by my earlier comments and leave it at that.
@Rob
Please update your research on ind ag, especially of course in China
Bats and pangolins often live together, they share caves, and viruses
Humans, in many countries eat pangolins (I guess this what you mean when you use the word ‘interaction’) and do domesticate them as well, at least in Africa they do – you would be hard put to tell the average jungle dweller that his eating of the pangolin is now ‘illegal poaching’ and ‘trafficking’ – they seldom appreciate men from far away calling them by such names of contempt
In low density and common habitats cross over viral infections to humans have been rare, although adoption of a city based lifestyle does cause pangolin meat consumption to inflict gout on more elderly clients
What has happened in China, contrary to your assertions, is an expansion of the old habit of catching and eating the pangolin into an industrial style farming of the animal, in close proximity not only to other farmed animals, but to the wild areas where bats live or in areas from which recently they have been displaced
It appears that in China there has recently been rapid expansion in pangolin farming due to a virus infecting pigs, creating a shortage of meat
Pangolin meat, you should know, is prized as tasty, he is a fairly easy catch
As for NZ, I was pointing out the failure of their policies ; however, given your admiration for such and your enthusiasm towards the imitation of these, and in light of your dismay over your country’s governance, I suggested you might wish to learn a lesson in practical democracy from Lincoln so that you could benefit your country with these same NZ policies
Debate is to exchange ideas and to learn about subjects beyond usual purvey – a learning process such as to dissolve and modify prior certainties assumptions and prejudices ; when you do not understand (or even if you think you do) it would be wiser not to employ accusations such as ‘dissembling’
The virus will disappear magically after 2020 Election. Same as war on Terror.
The actual national health crisis is the American diet. I’m as guilty as anyone, but if you want to show a graph of the death and health problems attributed to poor diet, it would be off the charts.
Or a dozen other things but right now its Covd.,
@Ted
Obesity is a major contributor to mortality in CoViD patients. It may be one of the reasons why CoViD has tended to cause lower mortality rates in SE Asian countries, where obesity is far less prevalent (although: of additional relevance in those countries is the fact that they have a much younger population in general — with the notable exception of Japan).
Also related to diet are diabetes and heart disease…both of which again tend to cause higher mortality in CoViD patients.
So you’re right in saying that the American diet is a national health crisis.
Another Trent Engine Issue ala XWB: ?
https://www.telegraph.co.uk/business/2020/08/11/rolls-royce-hit-engine-troubles/
Remember this was the tip of the iceberg on the Trent 1000. Reports of Trent 900 problems that have been hushed up (possibly the Super 900 that gained enormous SFC magically)
Don’t trust data you didn’t manipulate yourself.
Put that data into 2 perpectives:
1. plot it on population
2. plot it on the age of deaths
You’ll see CoV Sars2 is highly overrated in it’s influence, the USA didn’t had 330 mio. ppl. and those dying are old and sick, not young and healthy (compared to spanish flue or war).
Sash, you’re last point is on very dangerous ground: I can see exactly the point that you’re making, but others like to get emotional rather than rational when looking at this issue.
Here in the EU, the CoViD deaths were very heavily skewed toward over-70s with multiple underlying health conditions. The current uptick in infections in Europe is predominantly among younger people (20-54): interestingly, although infections are on the rise, hospitalizations are barely moving, and almost no additional cases are being admitted to ICUs.
As regards the POSSIBLE long-term health effects in CoViD survivors, people need to do a little more reading as to how PREVALENT (or not) these effects are among most of the population…and they also need to compare them with long-term health effects that arise following other medical conditions, including ones as “simple” as mononucleosis, giardiasis…and even pregnancy/childbirth.
I know 5 people who had CoViD. Only one died (84, with underlying issues), one was completely asymptomatic (96!), the others (70, 65, 55) had flu-like symptoms for 2 weeks, followed by post-viral fatigue for 2 weeks. The four survivors are up-and-running without any health issues. Interestingly, only one of them had measurable antibodies (IgG) a few months post-infection.
The IgG test is not a test of immunity, as the antibody response varies widely in recovered individuals. The true test of immunity is whether the body can marshal the same defenses again, quickly enough to prevent significant illness.
Statistically, the occurrence of COVID reinfection has remained extremely low, in the noise margin, after about 6 to 8 months of major infections. This implies that the body can & does learn an immune response. That in turn is a factor in favor of eventual vaccine effectiveness, if a suitable vaccine can be developed.
In the US, hospital resources are being strained by the resurgence of the virus. The impact is proportional to the number of new cases, as was also true in the first outbreaks.
It’s important not to select just those facts or articles that support a personal view. It helps to have a broad perspective using lessons learned around the world, both good and bad. There is a great deal of evidence available now, so the lessons are emerging pretty clearly. The question is, can we evaluate without bias so as to extract the maximum benefit?
1. It’s clear that precautions against the known transmission vectors are effective, and also that public cooperation with precautions is hugely important.
2. It’s clear that some activities and environments have higher transmission risk than others, such that we can adapt and adjust around those risks.
3. It’s clear that flattening the curve buys time and reduces the strain on resources and economic damage, allowing the maximal continuation of activities.
4. It’s clear that vigilance must be continued so as to avoid a resurgence, unless and until other control measures become available.
5. It’s clear that good leadership and consistent messaging is extremely effective and enhances public responsiveness and cooperation. In contrast, divisiveness and pursuit of unfounded personal beliefs creates confusion and a chaotic response, which ultimately costs lives.
6. It’s clear that a vaccine is desirable and beneficial, with reason to believe it’s within the grasp of our current knowledge and understanding. Therefore worth the investment for whatever we are able to achieve.
7. It’s clear that common recognition and acceptance of these things advances our knowledge and benefits everyone, with significant potential to save lives.
8. It’s clear that agreement and pursuit of common goals is far more effective and beneficial than argument over differences in evidence, which tend to scatter and de-focus resources and effort, producing highly differentiated results (and thus sustaining the arguments). Successes from around the world can be emulated and combined, and failures from around the world avoided, with a cohesive, open, learning approach.
I consider the reasoning in your second paragraph to be flawed…because you omitted to stipulate that it refers to KNOWN occurrences of CoViD re-infection.
With 40% asymptomatic infections, another 40% mild infections, and a false negative rate of 30% for the standard nasal/throat swab test, there are probably many CoViD re-infections that are remaining off the radar. Even worse: on an individual level, there is considerable socio-economic pressure to cover up a second infection, because most people can’t afford the work interruption and/or social isolation that an admitted second infection would entail.
Remember that we already have very adequate experience with another family of corona viruses, i.e. those that cause the common cold. For that family, re-infection is a regular occurrence, and a vaccine has never been developed.
Bryce, your assertion here is that re-infection is not evident because it occurs only in asymptomatic persons who have never sought medical assistance. Or that re-infections are being hidden by again not seeking medical assistance or testing positive. That’s a good example of the selective argument I mentioned. You deny what is true in favor of what you think should be true, as that would reinforce your personal belief.
Reinfection of the common cold virus occurs due to the large number of variations that exist (over 200 and counting), as well as the continuous change in the virus genome. That may happen with COVID as well, but as of yet there is not evidence of it. Several strains have been identified but all are similar enough to lend credence to a vaccine.
You argue against the viability of a vaccine, but that is quite far from the majority view of people who have far greater knowledge and understanding of the topic than you. So the world will continue to invest in the potential value that would result from vaccine research, even if only temporary and resembling the flu shot, and even in the case of failure. There is still something to be learned, as opposed to not trying, which is self-reinforcing because it ensures nothing will be learned.
@ Rob
I’m not “denying” anything: I’m merely pointing out that “absence of evidence” is not the same as “evidence of absence” — particularly in a situation in which only the tip of the iceberg is readily visible.
As regards vaccines: the Robert Koch Institute in Germany warned again today that, if and when such a vaccine comes, we should not get our hopes up as regards its effectiveness. Of course it makes sense to try…but it is folly to cling onto a Utopian hope in the face of multiple warnings from experts.
Management of this virus urgently needs a “Plan B”.
Bryce:
You are also discounting that its multiple vaccines being developed, not a single one.
Several lines of type as well, not all the same approach. Some very new and some old standby that works.
So, even if not a complete answer, an initial effective helps hugely, others get developed until there is an answer.
While its not a given, we are into this pushing a year (from initial) and no reports of it morphing fast either like flu does).
Ego, it may be a stable virus (like many others) we have to see. If stable then vaccines work.
This also is not a virus that co developed with people, its in a Virus interest not to kill, ergo colds, annoying but not fatal.
Which this one proves to be is open, but we are going after just a single base at worst. Not 200 variations of cold types (4 of which are Covd based)
Bryce, as I mentioned you tend to characterize things in terms that support your own beliefs, but are not supported in the wider body of available evidence.
The “absence of evidence” argument would require proof of a negative assertion, as to the lack of reinfection. It’s similar to “the truth is out there” reasoning. The evidence we have at present is that there are no significant numbers of reinfections. That could change if the virus mutates to a significantly different form. But at least for now, the consensus is that hasn’t happened.
Also the characterization of a vaccine as “folly” or “Utopian” is not supported by the progression of some candidates to Phase 3 trials. That would not happen for a hopeless endeavor. Those results will be important for continued assessment, and to better understand the potential for effectiveness. We’ll learn as we go, but those efforts are absolutely valid and appropriate.
As far as representation of the vaccine as a panacea, I have not seen any reputable source make that claim. The expectation is that a vaccine could add some degree of resistance to the general population. We don’t know more than that at this point, but the trials thus far are encouraging.
@Bryce
This report will interest you
http://www.scmp.com/comment/opinion/article/3097027/covid-19-hygiene-are-we-sanitising-our-way-next-health-disaster
All the measures taken to ‘contain’ or ‘limit’ infection have their price
All the more so lockdown, quarantine, isoaltion
@ Gerrard White
Thanks for the link regarding the potentially adverse effects of hand sanitization. We’ve been hearing similar sounds for years here in Europa, where an increase in allergies is being attributed to overly zealous hygiene.
Another point that is often overlooked: what is the number of increased deaths associated with other medical conditions that were discovered too late due to widespread lockdowns? In the Netherlands, it’s estimated that there will be an extra 25% cancer deaths this year due to delayed discovery — which translates to 9,000 cases. This exceeds the number of registered CoViD-related deaths (6500) in that country.
In a complex and interrelated biological ecosystem, turning one knob can (and usually does) have major unintended side effects somewhere else in the system.
@Bryce
I have understood that about allergies and indeed many diseases : we all have trillions of friendly bacteria on our skin inside our bodies which we should seek to preserve not wash or drug away
The bacteria are parasites in the same manner as is the virus, it does not seek to kill us, for in that way it loses house and home, it kills only the very weak, and this is by mistake
The immoderate consumption of anti biotics whether directly or via ind ag meat not only weakens the immune system but is said to be a prime cause for obesity
I have seen reports that many patients suffering from other diseases have deferred (or been deferred) treatment, which will now or soon result in increased deaths
And there is the basic point that a very high majority of deaths have occurred to those not only very old, but also very ill from other diseases or conditions
As you say it’s better to go at the problem from the other way round, mass obesity is a recent invention, as is mass cardiac and mass diabetes (and mass…) – restrain these and many if not most of the deaths associated with this virus will cease
“In the US, hospital resources are being strained by the resurgence of the virus. ”
Unsurprising if resources have been funneled to
lesser hit GOP controlled states away from the needier ones (big population centers) with DEM government by the Federal administration.
In effect killing off predominantly “undesired” ( for Trump winning in November ) voters.
I am aware that humanism never made it to the US.
But ..
‘Flattening the curve’ prolongs the agony.
Whatever happened to the desire for ‘herd immunity’?
People are dying waiting for surgery, dying afraid to go to hospital for help in the atmosphere of fear created by pandering panicking politicians and flappers, dying from suicide and intoxicant overdose. More will die from delays in diagnosis and treatment of problems like cancer, according to research. Which also shows reduction of life expectancy from the stress of joblessness – 40% of people who lost their jobs in this panicdemic are still out of work. The proper policy is one to minimize Total Harm, not eliminate what may linger around.
And to protect what feeds you – freedom. Politicians are quick to force you, as Canadian finance minister Moreau did in trying to extort from banks to get something he wanted – threatening them with a law change. And they lie, as Trudeau v1 did to invoke the War Measures Act.
For those who are clinging onto a hope (or delusion) that the SARS-CoV-2 virus behind the current CoViD outbreak is not mutating, it seems a reality check is needed.
The virus is an RNA virus (as opposed to a DNA virus), and all RNA viruses mutate. In a study published in April, scientists in China had already discovered mutations into 30 different strains…in just 4 months.
Some informative reading (out of many such articles):
https://www.newsobserver.com/news/coronavirus/article244093332.html
Bryce, as always you focus on the parts that support your view. This article is a reprint from the Atlantic, which when presented in full, reports accurately that although mutations always are occurring at some level, the vast majority are not significant to the function of the virus.
This is consistent with common sense and the developmental history of COVID. It underwent many mutations in multiple host species before the mutation that allowed the jump to humans. That one was obviously significant, but also required a long chain before it. Remember the mutations are random, the virus doesn’t have an ordered progression.
Something like that could happen again, but the odds are low. That’s why we have new diseases emerging over periods of many years. The article points out that the flu virus has a mutation rate 10 times higher than COVID, and the flu also evolves to both more and less virulent strains over time.
Finally again we have to look at the evidence we have, which is that there are not functionally different versions of COVID. And we know that immune responses are similar for variations of the same functional virus, and that variations of the virus are being studied as they emerge. So there is reasonable hope for at least some level of vaccine success. How much we don’t know yet.
“Finally again we have to look at the evidence we have, which is that there are not functionally different versions of COVID”.
That’s strange: the article talks explicitly about the G614 variant (in Europa) being “10 times more infectious” than the D614 variant (in Asia). But, of course, you overlooked that bit because “as always you focus on the parts that support your view”.
And now, you’ll treat us once again to a long sermon in which you repeat the usual list of “play safe, and don’t rock the boat” points…
The point is that nothing in the article points to the futility of a vaccine. That is your conclusion, which is consistent with your thesis, but is not shared by the authors or the scientific community.
The article states that one mutation is more contagious than the original, and has now dominated the infections around the world. But it also states there is not a change in symptoms, treatment or mortality rate, because the virus function is essentially the same.
Other articles discuss this in more detail. As new strains emerge, they are sequenced to look for changes that would alter virus function or infection method, because these would have implications for vaccine efficacy. None have been found thus far. This is why it’s widely believed that a vaccine is a worthwhile pursuit.
My “sermons” are against this misrepresentation of the truth. It has the potential to do a lot of damage. The virus is benign in it’s intent, but views like this are not benign, they are meant to sow discord and distrust. I have no doubt that some people will disbelieve or refuse an eventual vaccine, because of doubts such as this.
There is always room for factual criticism, but along with that is the requirement that the facts be followed, at least until they are shown to be incorrect.
If you want to say that there is a possibility of vaccine failure, that is true. If you say there is a probability of vaccine failure, such that the effort is not well founded, that is not true within the facts as we understand them today.
Interesting thanks.
Beware in general of premature research, some of it incredibly shallow.
(A US government agency used the term ‘underpowered’. Researchers often publish incomplete and premature reports to get publicity and funding, especially if the topic is hot. And activists/flappers misquote – in one case a university wrote a report about loss of farmland from a hydro-electric dam, clearly stating that a ground check showed the results of their analysis were plain wrong – but eco-activists keep reporting the results of the flawed analysis. And recall results of the fraudulent UK research on vaccine and autism are still be quoted despite widespread publicity about the fraud.)
Scott, you have to normalize for population.
US numbers of _cases_ sound large because the population is large compared to most generally similar countries, ten times Canada and Denmark for example, more than twenty times New Zealand’s.
It’s not _cases_ that matter, it is _deaths_.
There’s emotionalism not seen in past pandemics such as avian flu, swine flu, Hong Kong flu, and SARS v1. That’s dangerous for aviation which is the target of climate scammers, NIMBYs, and anti-business activists. Politicians pander – look at the US Cabinet Secretary who admitted having banned DDT without any evidence of harm, indeed a huge government study showed no harm. (and WHO is now recommending use of DDT against malaria-carrying mosquitos in some situations).
With media being a major problem – exaggerating, mis-representing, …..
Read up in http://www.moralindividualism.com/covidgov.htm.
Yes, it is deaths that matter and, while the US has a larger population, its per capita death rate is well over 100 times that of New Zealand.
Have a look at https://duckduckgo.com/?q=ourworldindata.org%2Fcoronavirus
Scott, waiting for vaccine that is safe enough is a fool’s game, you can’t predict how soon. (Wanna sign up for an MMA? 😉
Achieving herd immunity is a way, and it may be sooner than thought given the number of people who were infected but not reported, and the possibility that some people are immune for other reasons such as having antibodies for a different corona virus like SARS v1 and possibly some strains of INFLUENZA (the perennial killer) and even the common cold.
Recognize that SARS-CoV-2 is not a great risk for most people, the essential is shielding the vulnerable. Florida did that aggressively, Sweden eventually did that – without significant lockdown. Care residences and hospitals are where at risk populations are, by definition most people in care residences are in quite poor health. As with INFLUENZA, lung deficiency and heart deficiency are the big risk (heart essential to good lung function). Poor body function due to other things is also a risk, such as kidney and liver problems.
I challenge people to answer: “Is this pandemic worse than a very bad INFLUENZA season? (May be difficult to answer as statistics are suspect IMJ, for example Canada’s on INFLUENZA are suspiciously low, and COVID-19 death statistics out of Italy varied 8x. I suspect statistics on COVID-19 are falsely high, it is easy for busy people to just write something down – note the pandemic started here during INFLUENZA season, which can last well into spring. Is cause of death recorded as pneumonia, or heart failure, or an infectious disease that weakened an already impaired body?)
Otherwise know your own health – I know quite a few people who are self-isolating because of conditions like recent cancer treatment, a cancer growing very slowly, or still on suppressants from organ transplant.
PS: You read the ignorant flapping conspiracy theorist idiots in this forum, the same mentality is out there about SARS-CoV-2/COVID-19, some of them elected officials. Even those who are just ignorant herein are like certain ‘Health Officers’ who fall for the ‘modelling’ nonsense, couldn’t grasp why Italian hospitals were overloaded, and that care residences were the big risk in Italy.
AND: Get vaccinated against pneumonia bacteria, many if not most deaths with COVID-19 or INFLUENZA are from pneumonia taking advantage of weakened lungs.