Leeham News and Analysis
There's more to real news than a news release.



Bjorn’s Corner: Do I get COVID in airline cabins? Part 12. New results.
October 9, 2020, ©. Leeham News: We interrupt our series about hydrogen as an energy store for airliners to go back to our previous theme for a Friday or two: Do I get COVID in airline cabins?
IATA, Airbus, Boeing, and Embraer did a joint presentation yesterday about their latest knowledge about COVID and flying, and with the Pandemic entering the second wave in many countries it’s a timely subject.
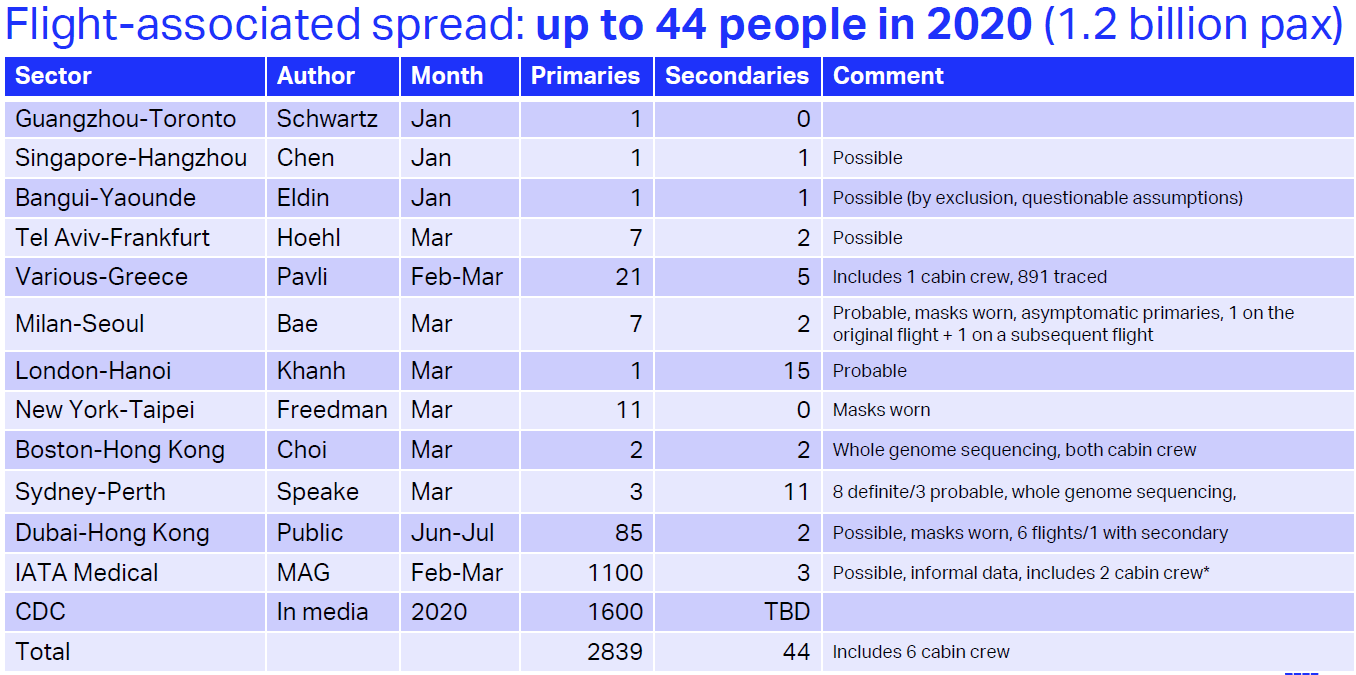
Figure 1. IATA’s statistics over 1.2 billion passengers flying with 2839 contagious persons on board. 44 others got infected during the flights. Source: IATA.
What’s the latest knowledge
When we covered the risk of being infected with SARS-CoV-2 in our series that ended 18 July we made several assumptions based on limited evidence around the risk of being infected while flying.
IATA (the airlines’ association) and the OEMs have been busy adding knowledge to what we could present in May/June/July. We have been briefed on their results over the last weeks and yesterday IATA hosted a webinar where it was all revealed. Let’s start with IATA’s statistics.
COVID statistics from airlines, authorities, peer-reviewed studies
IATA has been analyzing and collecting statistics on what can be plausible in-flight infections since the Pandemic began, Figure 1.
Of 1,2 billion passengers that have flown, IATA finds 44 plausible cases of in-flight infections. Observe that the statistics include the early phases of the Pandemic with March having the most infections of passengers during the flight (Secondaries) by infectious passengers who boarded the plane (Primaries). This is also the period when mask-wearing was not universally adopted.
The statistics are at the same level as the probability of being hit by lightning. But there is a probable rate of infections that are not in these figures. Here is IATA’s comment to the figures:
“The risk of a passenger contracting COVID-19 while onboard appears very low. With only 44 identified potential cases of flight-related transmission among 1.2 billion travelers, that’s one case for every 27 million travelers. We recognize that this may be an underestimate but even if 90% of the cases were un-reported, it would be one case for every 2.7 million travelers. We think these figures are extremely reassuring. Furthermore, the vast majority of published cases occurred before the wearing of face coverings inflight became widespread,” said Dr. David Powell, IATA’s Medical Advisor.
Our comments to the IATA figures
Readers of our Corners know we identified the largest risk when flying, not as during the flight itself but when boarding/deboarding. These figures include these phases.
Why are the infection figures so low? All three airliner OEMs have done independent studies of in-flight infection risks with slightly different methods. All three have used the advanced CFD tools they use when designing their cabins.
They have runs hundreds of simulations and studied the spreading of a coughing event from an index passenger (called a Primary passenger in Figure 1) to other passengers back and forth.
The OEMs’ results
The OEMs have all three reached similar results. We will go through them in detail and present their methods and figures, but here a summary of their findings:
- The likelihood of being infected by a COVID infectious passenger coughing in the seat next to you in a single-aisle airplane (no empty seat between you) is lower than if you sat/stood 6 feet apart in your office/home/shopping center (in both cases masks are worn).
- If the infected person spreads 10,000 infectious droplets of varying sizes (from large droplets down to aerosol size droplets (which are 1-5 um)), you will worst case get 5 inside your mask. You get ~10 if you are 6 feet apart with masks.
- To be infected with COVID you need a much higher viral load than this. IATA and the OEMs stay clear of the viral load discussion as this is for medical experts to debate. Our findings are; a critical viral load leading to a probable COVID infection is magnitudes higher than these figures.
- The masks simulated are of the common types, not the high-grade N95 type.
- The results are the worst cases of hundreds of simulations.
- Boeing has also done flight tests with cougher and breather dummies in a 737. Same results.
The results from all three OEM confirm what we said May to July in our COVID series. The risk of being infected in-flight is very low. Even if you fly for hours. We shall note the OEM simulations cover the flight phase. This is what they control by their cabin environment.
The risk of being infected during the complete flight (including boarding/deboarding) is higher, but still low. IATA’s statistics cover the whole flight, boarding, flight, deboarding.
Passenger fears
IATA has research that shows 80% of passengers fear sitting next to a COVID infectious person during the flight. This is the primary fear.
The next fear is touching a surface where an infectious person has left viruses that you can get COVID from. As we have written before, we have yet to find a study that confirms infections via the contact path.
This shows we cannot follow our instincts when it comes to COVID infection risks. We focus on the low-risk areas and disregard the high-risk ones.
We have referenced simulations that show the boarding and deboarding phases as the high-risk phases when flying. Boarding and deboarding are procedures where the airlines make all the difference. Their procedures and discipline executing these must now be the focus going forward. They suffer from the non-flying of their customers and they hold the key to getting customers to return to flying with confidence.
We must quell the type of headline-grabbing articles in our media where a half-baked University CFD simulation shows how we all get COVID during flight. The evidence from our OEMs shows this is indeed not the case. This shall now lay these kinds of articles to rest.
Thanks Bjorn, it’s good to see these analyses. Almost all of the negative reporting had referenced the same few studies conducted after the original SARS outbreak. Now at least we have current studies and data involving COVID directly.
The next challenge would be the world working together to establish better protocols to reduce the need for quarantine when traveling. That’s a far more difficult problem but it will be essential for air travel recovery.
You still need Quarantine with a test 5 days after travel. That reality is 7 days allowing time to get the test results back.
Only a vaccine is going to negate the need for that.
Air Travel just has to live with that until we get there.
The vaccines are coming, and the latest serious guidelines will be followed not rushed. We can hope early Spring for a good start and mid to late summer for a majority.
Once Fauchi gives it his ok I am in line (yes I will be watching others but I use him as the gold standard)
It’s unwise to pin all our hopes on vaccines…there needs to be a plan B.
And there needs to be a re-examination of strategy while we’re waiting for vaccine introduction (if an effective vaccine comes at all)…otherwise, we run the risk that mass CoViD fatigue and insubordination will de facto put a new strategy in place anyway.
The governments in IRL and NL recently rejected advice from their respective CoViD management teams regarding stiffening of mitigation measures…so there are some indications of a move away from the tunnel vision that has dominated up to now.
Here are some recent insights on mutations/vaccines:
https://www.hospimedica.com/covid-19/articles/294784719/sars-cov-2-mutations-having-higher-transmission-rates-could-require-yearly-covid-19-vaccine-shots.html
+1. We may never have a vaccine. What’s going to get us back to normal will be rapid testing (and by that I essentially instant), effective treatment so that symptomatic COVID isn’t perceived by so many as 100% fatal, and recognition that preventing COVID deaths almost certainly increases death from other causes, and that we need focus on minimizing how many people die, not how many die of COVID.
These are only the cases that have been traced, so they likely to be a massive underestimate and you still have to get to the airport and stay in a hotel, etc. How can they tell if someone caught covid19 in a plane or while on holiday?
Figures from Hong Kong indicate that public transport is much less dangerous than originally thought.
Surface transmission seems to be less likely than originally thought.
Masks seem to be much more effective than originally thought.
Research also seems to show that shouting is a major issue.
The most recent data from Europe (probably commensurate with other countries) is indicating that risk is highest for (the combination of):
– prolonged indoor gatherings (particularly family settings);
– with poor ventilation;
– without face masks;
– with shouting/singing/rowdy behavior…particularly when alcohol is involved.
Although flying qualifies as a “prolonged indoor gathering”, the other points are (generally) not satisfied.
Yes, often if you can remove on part of the catalyst it works.
Aircraft are unique in layout and flow vs a room that is just intended for overall ventilation and requires each room to have its own study.
I will add in shouting for any reason is a bad thing.
@Grubbie
The figures look fantastically, or suspiciously low – 1.2B pax results in 44 infections, only?
As far as I remember early on at least and subsequently in many countries large numbers of pax did not wear masks – were they too spared?
Or were they counted out, excluded, from this survey? If so, how?
Statistics were kept for those who wore and for those who did not wear masks? – This seems un likely
How have the OEMs managed to t&t with any degree of likelihood let alone certainty that this pax and not that pax contracted the virus in the plane and not elsewhere?
There appears to be no explanation given from the OEMs as to why sitting in this closed space is many millions of times safer than sitting in all other closed spaces
Safer perhaps, to a degree – but to this exceptional high level of safety?
To believe the OEMs It is now impossible to imagine a safer place than an airplane, which is extremely counter intuitive
Safer because of superior airline ventilation systems, but they have compared say (worldwide) average office/ restaurant ventilation systems with airplane? And come to such a conclusive result?
Conclusion – Flying is ok, Yet offices metros restaurants churches etc are to be closed worldwide?
End result – if the public is to believe flying is made so quickly and without , evidently, massive installation of comprehensive intensive care style sanitary systems, the public is going to say ‘if making flying safe is so easy, how come shops offices ….can not be as easily made safe’
I’m thinking that the public will take two attitudes to these figures, if they are ever popularised – that either they are not credible, or if they are credible then all other measures (beyond those taken in planes) taken are reduced to worthless
The basis now is both statistical and scientific, in terms of nasal/oral droplet dispersion. That is the key metric for spreading events.
Airliners with people wearing masks have been evaluated, and there is not evidence of sufficient viral load transfer to support widespread infection. That is also the key difference that occurs in other venues, where there is sufficient transfer to spread infections.
As with all science, people may choose to believe the results or not. Anyone who is not convinced, doesn’t have to fly. But the science itself should not be denied in defense of their beliefs. If the science is viewed as incorrect, then evidence of that can be presented, and is always welcome.
@Rob
Can it be explained why the ‘viral load’ is so much lesser in airplanes than elsewhere?
Reason is required – the ‘science’ regarding this bug and transmission is already definitive?
This is doubtful – for We know so much yet can do so little to stem the increasing numbers of the dead?
In what sense can the statistics in this report(s) be considered faultless?
How can these OEMs show the 44 pax they identify contracted the virus in an airplane? How can they show they can not have missed any others out of the 1.2B
The report is a commercial commissioned report with an obvious vested interest – when science is bought and paid for it is reasonable to remain skeptical
An important added parameter that was found in the OEMs simulations and tests was dispersion. We have only counted displacement so far (the downdraft). When the OEMs could trace the path of each droplet they saw that dispersion is very important. It precludes a critical load to pass the masks of a neighbor as the concentration very quickly is diluted. This works with the laminar flow but even better with turbulent flow.
This is also why gaspers on or not, or shields like suggested by seat manufacturers didn’t really change the results. This was a new finding from these very detailed simulations and tests.
You have the same effect in other windy situations where there is no re-entry of the air.
As Bjorn reported and I mentioned, the studies’ discovered droplet exchange rate was not enough load to lead to infection.
If you have evidence to the contrary you are free to present it. There does not appear to be either statistical or scientific evidence for that, at this point.
“Can it be explained why the ‘viral load’ is so much lesser in airplanes than elsewhere?”
Yes. The air exchange rate in airplanes is exceptionally high (2-3 minutes) and aircraft ventilation systems move “droplets” vertically instead of horizontally, which rapidly gets them away from your eyes, nose and mouth. It’s always good to be skeptical, and with respect to the numbers of infected, “modeling” hasn’t served us especially well during this affair, but the design of aircraft ventilation systems is well established, and how that affects COVID dispersion is fairly easy to determine.
There’s very little science involved here, it’s more like religion. Where does the 90% higher number come from? It’s just a guess based on nothing more than wishful thinking.
Poor discipline alone would seem to be likely to cause more transmissions. Or is the fact that older people are not flying mean that there are more asymptomatic cases? Who knows?
Anything less than many thousands of transmissions is implausible with current knowledge.
Grubbie, this work was scientific, there are articles published showing the masked and instrumented test dummies seated in airline cabins, with coughing/sneezing/breathing mechanisms and droplet tracing to surrounding seats and rows.
The scientific data supports the statistical data. At this point there is not evidence to the contrary, as far as I know.
This data further enhances what we already knew/suspected.
As I said before, I know lots of people who have no issues with taking a flight…the problem is that their desired destinations all have quarantine-on-arrival requirements, which is a killer for anything other than long family visits.
At least one country sees that this needs to change — Singapore is exploring ways to re-open the country to air travelers, on the basis of (repeated) testing rather than quarantining:
https://www.bloomberg.com/news/articles/2020-10-06/singapore-races-to-open-borders-warning-its-future-is-at-stake
It might work for Singapore but you have to have rapid turn around and daily tests and tracking. US would not work at least in the current climate.
Your originator trafficked needs to have the same rigorous ops.
No easy answers.
Did a lot of airport workers that interact with passengers get sick before air travel traffic dropped? Ticket agents, gate agents, security screeners, shuttle bus drivers, etc?
While its locale, I have not seen reports of that in our area.
There is a major use of plexiglass to prevent direct paths, masks, physical distancing.
I would like to see more about the numerator – for instance length of flight, proximity of the secondary passenger to the primary, level of contagion in the place of departure.
The denominator of 1.2 billion people is ridiculous. It would make much more sense to make the denominator the number of people on the flights where disease was transmitted. I already know I can’t catch COVID-19 on a flight where no one is infected.
@Stan Sorscher
They have no other figure than 1.2B, besides this suits them
They do not know how many pax flew infected, they do not know how many flights included no infected people, they only claim to know how many deaths their statistics can attribute to air travel
As I understand this – What they wish to claim is that of the 1.2B many, an unquantifiable number, flew infected, yet nonetheless transmission was low
This is including the circumstances where many flights were somewhat or even largely maskless – although I suppose that there can be no statistics recording how many masked and how many unmasked compose their 1.2B
Gerrard, the article shows 2839 infected people as the primaries, meaning already infected when they boarded the flights where infection is suspected.
Then it shows 44 secondaries, as people who are suspected to have became infected in those flights. Note that deaths are not discussed at all.
Since only flights where infection is suspected to have occurred are considered, we cannot say the primary count is all the primaries that have flown, out of the 1.2B total passengers. That number is probably much higher. However as far as we know, those other primaries did not cause in-flight infection.
@Rob
The study shows 2839 infected people flew in airplanes out of a quoted total of 1.2B pax?
‘where infection is suspected’ – this is unscientific let alone ridiculous – on what grounds can a study of transmission be made if the study deals only with those situations in which it is suspected – rather than it is certain – that there may be, or not, infected pax flying
Who is doing this suspecting? – in no other circumstance can one suspect someone of being ill unless it is to proceed to establish whether he is or not
One might more reasonably suspect that all flights might have carried infected pax, or at least one might suspect it is unreasonable to select those we want to suspect did and by the same suspiciousness to suppose that certain flights did not
The results conclusions of this study can not be an accurate – of course there will be few transmissions and hardly any deaths if so few (suspectedly) infected people fly
If, on the other hand, many more infected people flew than the famous 2839, (out of 1.2B one can say that it is reasonable to posit a figure of several magnitudes higher – but of course this would require a seriously constructed study to establish) some of them, at least, must have transmitted infection, but all these pax are outside than parameters of the study
There is still no answer as to why transmission is so much lower in airplanes than it is held to be everywhere else
People sitting in an airplane seat, even dummies, transmit less than in any other situation? Why?, or how?
All you say is that the study shows this to be the case – but a study with such faulty methodology and with such blatant commercial interests to seek to defend is not ‘scientific’ nor authoritative, indeed raises suspicion in the minds of the suspecteds – that is to say the rest of us
Studies like this give what is called ‘science’ a bad name
Bjorn:
We had a family crisis that dictated two at risk family member travel, one way up on the risk end of age.
With your reporting, I was able to let them know that if we could manage the departure and arrival end, it was viable, not risk free but could be done generally safely (probably safer than a trip tot he grocery store)
Limited exposure going to and a direct pickup at the airport on arrival on both parts of the trips. They stayed seated until the aircraft had cleared.
The protocol used was a test before, then quarantined, test 5 days later after arrival.
Only one on the return but followed the same guidelines.
Neither r one contracted it.
While that is not relevant statistic wise it also is relevant in how to use the information the mitigate the risk. Enough data and you can determine the degree of risk.
People can argue the edges of the data, but overall its proven to be solid.
Testing alone is not the answer (as we have seen) we still need the quarantine for safe, but it can be shortened to a week if you test negative.
Use the masks as well.
Its a system and it can and does work. Where it fails is where people think they are special and ignore it (congressmen for Missouri) or the President as a poster child of how not to do it.
Bjorn, I’m a bit disappointed that you have gone with this. Would you really recommend that older relatives fly at the moment? It’s a bit dodgy at the best of times, with the flu and DVT.
I would agree that it’s not as dangerous as at first thought.
My Mom needed to fly as did my brother. As the boys are all over 60…….
We did not ignore it was a risk but the other aspect was a really bad thing so we went with it.
That said, do I recommend it? Only if you really need to.
@Grubbie
Surely what your older relatives do is their own responsibility…not Bjorn’s?
If your older relatives easily suffer from sunburn, will they themselves take the initiative to use sunblock, or will they first wait to see what Bjorn says?
In GENERAL (at least in Europe):
– People under 40 suffer minimal symptoms from CoViD, and virtually no mortality — unless they are obese and/or have serious underlying medical conditions. They can take solace from this data.
– Similar considerations (though somewhat less rosy) apply to people in the age range 40-55.
– People above 55 need to use their own common sense in deciding what risks they do or do not wish to take. Their effects from CoViD tend to be significant, though nothing like the situation for people over 70.
– And people above 70 need to adopt an attitude of minimal unnecessary exposure for the coming months.
There is no “one size fits all” solution to the current problem.
Looking at the Dubai-Hong Kong data from June/July, there were 85 primaries present on 6 flights…which corresponds to an average of about 14 primaries per flight. If we assume a widebody with capacity for 300 pax, but only half full (typical at the moment), then about 1-in-1o passengers on board was a primary…which is impressive! Even if the flights were full, it’s still 1-in-20, which is still impressive.
In fact, seeing as CoViD PCR tests are at least 20% false negative, the actual numbers of primaries were probably even higher.
https://www.abc.net.au/news/2020-07-15/covid-19-testing-not-as-accurate-missing-coronavirus-cases-grow/12455076
On the other hand, a recent study in the UK suggests that as many as 86% of CoViD-positive people do not have a cough in (at least) the first few days of their infection. A lack of coughing greatly decreases the risk of spread in a situation in which everyone is wearing a mask (and visor, in the case of Qatar Airways) and quietly sitting stationary…particularly with the efficient ventilation in a plane.
I have seen the test results from Teague and many others on cabin airflows. Airstream are going sideways and upwards on place you don’t want. Refreshment rates are just averages.
Embraer even contradicts their own (pre Covid) observations.
https://www.embraercommercialaviation.com/clean-air-clean-cabin-safe-flight/
The OEM’s, the airlines and their IATA are far, far from independent on this matter. Because they are in survival mode. To prove the source from infections is hardly possible also in aircraft cabins.
The industry has put up a media wall everything is ok. Closely guarding any cracks.
If I would place 5x airline 4 seaters in a walking street and put 20 people, shoulder to shoulder, 30 inch pitch, for hours, I probably would get arrested.
OEM’s useally only ackowledge a problem after there is a solution.
Good points.
Plus: people remove their masks in order to eat/drink during the flight.
Plus: masks can slip aside, or fall off, unnoticed while people are sleeping.
Plus: we have no idea what people are doing mask-wise when they’re in the lavatory. Is the lavatory on an aircraft ventilated as efficiently as the seat area? Aerosols can hang around in an elevator for 40 minutes.
Nevertheless, because of the general ventilation patterns on board, I’d rather take my chances in a plane than in a theater or congregation hall…or crowded subway.
@Bryce Usually I agree with you, but
You can leave/change seats a theater, you can leave a hall, you can leave a …if you do not feel well, if you suspect someone nearby is sweating mask awry or sneezing or….for any reason you may have to think it may be better to leave than to stay
That is to say you remain the judge of your circumstances for good reason
But in a plane…..you are the prisoner of these same OEMs or IATA or airlines who commission PR for profit and try pass it off as ‘science’
I agree with all the points that you’ve raised.
For me, it’s a purely personal matter: I’m not afraid to fly…indeed, I flew to Asia in February, at the height of the outbreak there.
The reason (and we’re both in agreement on this): for most people, this virus does not pose a significant health risk, thus obviating the need to cower and fret in a corner. I observe the anti-CoViD measures that are in effect in my surroundings, but apart from that I get on with my life. Risk is inherent to life: anyone who’s not willing to accept that might as well become a recluse.
@Bryce I’ll agree with you on the risk
I read yesterday that the average age of deaths from this in England was 84 – in general in Europe it seems to go from upper 70’s into early 80’s
And we are not talking about the legendary fit and spry oldster here, but those already badly inflicted with other maladies
So there’s little to not much risk of either death or serious damage to anybody other than this venerable group who have probably dun roaming most of them
Life without risk is like an airline without mendacious PR, unimaginable
@Gerrard White
Same pattern in NL: the average age of CoViD deaths is 80 (for men) and 84 (for women)…and most (at least 75%) have multiple underlying conditions.
Obesity is a very significant complicating factor: although about 15% of the adult population in NL is classified as obese, 80% of the CoViD patients in ICUs here are obese.
Here’s a graph for Italy, showing recent demographics of CoViD deaths:
https://www.statista.com/statistics/1106367/coronavirus-deaths-distribution-by-age-group-italy/
And here’s some equivalent information from the CDC in the US:
https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html
It may be more accurate to speak in terms of the disease propagation vector. The path of COVID to reach the vulnerable population is through the non-vulnerable population. This was the lesson learned early on by Sweden and other locations, including the US.
We now know that vulnerability (especially with regard to fatal cases) is due to an uncoordinated immune system response, which lacks the normal multi-component system of checks and balances. Although it is predominant in older people, it can occur for various reasons, in younger people as well. There is no way to tell who might be affected.
I consider myself to be in the non-vulnerable population, as I’m healthy and have no risk factors other than age. I’m not afraid of contracting the virus. But, I don’t want to be part of the propagation chain that delivers it to others who might be vulnerable. So by protecting myself, I protect everyone else as well.
That is what’s wrong with the fallacy presented by Trump. He has disregarded precautions and held a super-spreader event at the White House. He contracted the virus, was hospitalized and given an experimental antivirus cocktail, for which he is not eligible as a participant of the clinical trials. This was done on compassionate grounds. He was also given over two times the normal dose, the cost of which in the trials is over $100K. This means he was given $250K in medicine alone. My guess is the cost of his recovery, to the taxpayers, is well north of $1M.
Then he emerged from the hospital, talking about a cure, and telling people not to be afraid of COVID, it’s not a big deal, he beat it. Yet he knows his standard of care was well beyond the means of most people, and he said nothing whatever about how or why he got it, or the importance of precautions, or the true cost of recovery and the implications of that for others.
This theme is similar to and consistent with looking out for himself first. It’s a selfish attitude, which he seems to wear with pride.
The irony is that if he took this seriously and really tried to help people by example, the infection rate could be slowed and more activities could be resumed, again by observing precautions. Trying to achieve that by minimizing the problem is counterproductive, as is now evident even within the White House itself. We should all learn from that, even if Trump doesn’t.
The actions and acceptance of Trump’s Covid-19 adventures, policies over the last 8 months months is hard to comprehend.
Imagine B Obama had held this super spreader event at the WH, ignoring advices, tweeting untruths non stop. How would the more conservative part of the US population have reacted? Demanding putting him in a hospital, jail?
The problem with the “infection must obviously be occurring” view is that there hasn’t been evidence developed to support it, either statistically or scientifically.
On the other hand, there is statistical evidence to support a very low rate of infection, and now a scientific basis for that result has been established.
As we so often see, the counter-argument is based on the view that the existing evidence is not valid, and the lack of counter-evidence is due to the industry concealing the truth out of self interest. So basically this is the elevation of an opinion over the observable fact, with a justification of bias on the part of others.
Another way to state this, is that the truth is out there, but it can’t be established because the “powers that be” prevent that from happening. That’s entering into the realm of conspiracy theory.
If we follow the scientific method, then we accept the available evidence, and if we doubt the data, mechanisms, or their veracity, then we propose experiments to test them.
So I would ask, what experiments or data should be pursued to develop evidence for the counter-argument? We already have statistical data, we already have droplet dispersion studies. What else should be done?
Apart from evidence, there’s also logic and deduction: indeed, many of the great discoveries in science (such as Relativity theory) would not have been made in the absence of deduction.
In the current environment, we know from multiple studies that at least 40% of CoViD-infected people are asymptomatic; in other studies (such as a recent one in France), 65% of a test group were asymptomatic. So, in a thought experiment, if a given group of 1000 CoViD-positive persons causes 100 follow-on infections, then (statistically) 40-65 of those follow-on infections will be aysmptomatic…and they will not show up on the radar in regimes in which only symptomatic persons are tested.
Coupled to this fact: the PCR test widely used to test for CoViD is at least 20% false negative — so we have even more infections occurring off the radar.
Inter alia for the reasons above, the CDC estimates that the actual number of infections is 6-24 times higher than the registered number of infections. The WHO is using a factor 20…hence its estimate last week that 700 million people have now had CoViD, even though only 36 million was the official tally.
So it is perfectly valid to expect that the actual numbers of infections in the studies above are much higher than the registered numbers.
Those uncertainties are valid, but they don’t alter the conclusion that air travel is safe.
In order to be relevant, the uncertainty in infection rates must be somehow more consequential in airline travel than in other social interactions. Yet the evidence we have from the certain infection data, is that it’s far less consequential. There’d be no reason to extrapolate a different outcome in the uncertain data.
Even in deduction, there has to be a reasonable basis, and following development of evidence. So again I would point out that there is no evidence at present, for the allegation of significant infection rates for airline travel, that could be used as an argument for restriction on such travel.
Relativity was a magnificent example of deductive reasoning by Einstein, but almost immediately confirmed mathematically by Special Relativity. Then again later by solving the much more difficult equations for General Relativity. Also in every test that has been devised thus far, Relativity is upheld by the evidence.
Einstein proposed many of those tests himself, even though the technology would not become available for many years. His deductive skills did not supplant the scientific method, but they allowed a substantial leap forward.
“Apart from evidence, there’s also logic and deduction: indeed, many of the great discoveries in science (such as Relativity theory) would not have been made in the absence of deduction.”
You’re right. Logic and deduction are excellent tools to propose hypotheses to explain observed phenomena. They’re, by definition, inadequate tools to confirm or repudiate a hypothesis. The only reason why we all accept the theory of relativity as being a theory is because every experiment done in the past one hundred years confirmed that the universe behaves in accordance with it. Actually, I’m sure that Einstein’s deduction went against what most people at time thought was logic or made sense. Heck, even today, most people’s reaction once they’re explained how spacetime dilation works is of initial disbelief. So I don’t think that citing Einstein supports your point, quite the opposite. You’re the one that is choosing to ignore the evidence and deciding to stick with what makes sense to you.
What I see is that there’s currently lack of evidence to support your hypothesis that air travel is risky from a transmission standpoint. Conversely, this article states that there is growing evidence to support the opposite.
@Rafael
I didn’t say anywhere that air travel was risky…you need to read a little more carefully.
I merely used deduction to posit that the actual infection rates are higher than the observed infection rates…usually by a factor of about 15.
I didn’t “hypothesize” that that increased rate detracts from the conclusion that air travel is safe: in fact, if you read my other posts here, I state quite the opposite.
A multiple of 20x seems ridiculous and unsupportable. Currently there are 215k deaths, more or less, in the US. If we use the early CFR from South Korea, which is much lower than the US CFR, then we get 30 million people who have contracted Covid, a multiple of less than 4x.
The weird thing is that you’re using a higher multiple as a sign that flying is more dangerous. If the actual number of infections is 20 times the “registered” numbers, then the US would be quickly nearing herd immunity with over half the country having already contracted it. And it would mean that despite perhaps 10s of thousands of people flying with Covid, we would have seen few outbreaks resulting in deaths, suggesting that the risk is even lower than expected.
This result is highly suspicious. Every frequent flier probably has stories of getting sick after taking planes. Using 1.2B pax as denominator is clearly ridiculous. The risk that should be simulated and presented is what’s the likelihood of a single carrier infecting other passengers. Dummies do not sneeze, cough, wipe their nose … Super-spreading events on board aircraft is well documented during SARS. Both SARS and SARS-2 are single strand RNA viruses with diameter of about 80-100 nm. So SARS-2 is some how safer than SARS makes no sense. Because air is so dry on planes, the large size aerosols will quickly dry and become smaller air-borne particles and can stay long. It depends on the efficacy of the surgical mask, HEPA and particular seating position of the carrier, and relative distance to high-risk passengers.
The article gives 1239 as the number of primaries on flights which are believed to have produced the 44 suspected secondaries. It doesn’t give the total number of primaries that have actually flown on all flights, because many of those didn’t result in secondaries.
Also the CDC does not give numbers for the secondaries, resulting from their 1600 primaries. If we scale from the other results, there would be 60 additional secondaries from that group, out of the 11,000 people the CDC estimates travelled with a primary. That brings the total to 104 secondaries.
It’s also notable that the CDC estimate of exposure was 11,000 passengers out of 214M that flew in the same 8-month period. So that is an exposure rate of 0.005%.
Further as Bryce pointed out, the primaries are those who were likely symptomatic and tested positive on arrival, or in quarantine. The actual number of asymptomatic primaries that have flown is probably much higher, but we have no numbers for that.
The bottom line, though, is that a very small number of documented infections have resulted from flight worldwide, from an equally low rate of exposure. Even if you assume a 90% underestimation, as the article does, these rates are still very low.
Yes, as the pandemic mounts, the articles saying, it is okay to keep doing something, in this case airline flying and the fliers will not get sick. Suppose each person had a separate air supply. Complicating details are equipping a steward(ess) or someone using the restroom, but no possible virus communication. Instead we get an argument that avoids refitting the aircraft.
One can come to a conclusion about anything from statistics by avoiding the whole picture. Everyone in this pandemic is saying people do not get sick from me or you cannot prove it. I do not see the article exploring a correlation between the number of flights and air travelers and the ensuing number of patients and deaths, perhaps in a stated time period. Standard fare for a statistician I would say.
The CDC does in fact give the data for number of flights (1600) and air travelers potentially exposed (11,000) out of 214M passengers in the same time period. They do gather information on individual infections but don’t release it as part of these studies, possibly for privacy reasons, and also uncertainty as to whether infection incurred before or during the flight.
The data that would deterministically resolve the question are not available, so statistics are the what we have to use. The statistical evidence is that clusters or super-spreader events have not been traced back to flights, whereas they are frequently traced back to other social gatherings.
I don’t think that avoids anything, it’s just the reality of the data we have. No other data have been bought forward to contradict this result.
No, you’re wrong here.
If you’re calculating your odds of getting hit by a drunk driver, you don’t only count those who are driving next to those who are drunk. If you’re calculating your odds of getting attacked by a shark, you don’t only count those who are swimming next to sharks. You count those who are driving in the former and those who are swimming in the latter, without having to account for whether there were drunk drivers or sharks.
Same goes for flyers. You count all flyers. And that’s how it should be because you’re not going to know whether someone has Covid on a plane with you, since presumably only those who are asymptomatic are going to be allowed to fly.
That said, epidemiologists do calculate the attack rate of a virus in various circumstances. Here’s a study showing that with SYMPTOMATIC Covid patients the attack rate was about 5%, which puts it significantly lower than things like eating in a restaurant, going to church, going to an office, or taking public transit. (The highest being living with someone.)
Thanks for getting back to real questions of today, instead of eco-double-fantasy land.
As for putting false claims to rest, don’t get your hopes up too high – you’ll dampen them, hopefully substantially, but true believers don’t listen. Look at the current US election campaign with its ranting lies, look at alarmists who deny basic physics of greenhouse gases and deny actual data.
This should have been headline news in all the media today! Out of 1.2 BILLION passengers only 44 confirmed cases on onboard transmission of Covid-19? It would seem being on board an airliner is the safest place to be during a pandemic (as many people got infected in the Rose Garden) and yet the industry has been decimated? Boeing, Airbus, Embraer, and IATA need to fund a major Ad campaign to educate the public on how very safe it is to fly today. There is no reason why airports should be nearly deserted right now.